Perimenopause is one of the most complex and consistently underaddressed biological transitions in women's medicine. This narrative review introduces the Perimenopause Chain: nine interconnected biological systems — circadian clock, sleep architecture, HPA axis and cortisol rhythm, insulin sensitivity and metabolism, cardiovascular function, collagen and connective tissue, muscle mass and body composition, neurological stability, and thyroid function — each governed by two master signals: sex hormones (estrogen, progesterone, testosterone) and thyroid hormones. When either governing signal becomes dysrhythmic, the chain weakens link by link. The chain is only as strong as its weakest link.
A central and non-negotiable principle: no dietary supplement restores hormones. The HRT triad — bioidentical estradiol, micronised progesterone, and testosterone — each contribute distinct, non-redundant biological effects that no supplement can replicate. The clinical laboratory protocol for perimenopausal assessment is presented with 29 reference values comparing standard ranges against optimal perimenopausal targets. Six theoretical intervention models (M1–M6) compare expected chain outcomes. A 30-day pilot observational study (N=20) provides preliminary hypothesis-generating data. A patient quick-reference guide translates the clinical framework into practical tools for the consulting room.
No dietary supplement restores hormones. HRT is the only intervention that addresses the governing signal. What chronobiological supplementation can do — when designed around the correct biological diagnosis and delivered at the correct circadian phase — is support the biological infrastructure that hormonal dysrhythmia has weakened. These are different tools for different levels of the same chain. Not competing alternatives. Layers of a coordinated framework.
In material science, the tensile strength of a chain is determined not by its strongest link but by its weakest. This principle describes, with remarkable precision, the biological reality of perimenopause. The perimenopausal body does not fail in one system — it loses coherence across multiple systems simultaneously, systems previously synchronised under the hormonal architecture of the reproductive years.
Standard clinical practice treats each consequence as a separate problem. Sleep medication instead of hormonal assessment. Antidepressants for neurosteroid withdrawal syndrome. Dietary advice for a condition driven by declining GLP-1 secretion and insulin receptor dysfunction. Dermatological treatments for a fibroblast cofactor deficit operating in a narrowing circadian window. The chain is addressed link by link, without addressing the mechanism of chain weakening.
This review is written for three audiences simultaneously: the menopause specialist seeking a comprehensive mechanistic synthesis; the general practitioner who sees perimenopausal women daily and needs a practical clinical map; and the perimenopausal woman herself — who is intelligent, motivated, and frequently better informed than the healthcare system that is supposed to support her. All three deserve the same complete picture.
The perimenopausal symptom constellation appears fragmented because medicine treats it as fragments. When mapped to the nine chain links, a coherent pattern emerges:
- Sleep fragmentation, waking 2–4am (Link 2): Progesterone decline removes allopregnanolone — the GABA-A modulator maintaining inhibitory neurological tone. Simultaneously, flattened circadian amplitude delays melatonin onset.
- Hot flushes, vasomotor symptoms (Links 1, 3): The hypothalamic thermoregulatory centre sensitised by estrogen withdrawal. Norepinephrine pathway lowers the sweating threshold. One of the most consistently undertreated perimenopausal symptoms.
- Mood instability, anxiety, neurological hyperreactivity (Links 3, 8): Allopregnanolone declines. A neurosteroid withdrawal syndrome producing anxiety and emotional volatility. Frequently and incorrectly managed with antidepressants before hormonal assessment.
- Genitourinary syndrome of menopause — GSM (Link 6): Vaginal dryness, dyspareunia, urinary urgency, recurrent UTIs, urogenital atrophy. Unlike vasomotor symptoms, GSM is progressive — it worsens without intervention and does not improve spontaneously.
- Cardiovascular risk escalation (Links 4, 5): The perimenopausal period — not post-menopause — is the cardiovascular risk inflection point. Estrogen cardioprotection withdraws, Lp(a) clinical expression amplifies, blood pressure rises.
- Skin, collagen, and connective tissue change (Link 6): Skin collagen 30%+ decline in the first five years after the final menstrual period. Joint capsule laxity, pelvic floor structural change, increased injury risk, bone matrix loss.
- Reduced exercise tolerance and slow recovery (Links 3, 7): Estrogen supports anabolic muscle signalling. Its decline raises the anabolic training threshold and extends recovery requirements. This is hormonal withdrawal from the anabolic support system — not deconditioning.
"You are not falling apart. You are not ageing prematurely. You are experiencing a predictable, biological, mechanism-driven transition — and the symptoms you are experiencing are signals from a chain that is losing coherence, link by link, because its governing signals are becoming erratic."
The nine links are presented in order of biological hierarchy, beginning with the circadian clock — directly governed by estrogen at the suprachiasmatic nucleus — cascading through the systems whose function depends on intact circadian signalling.
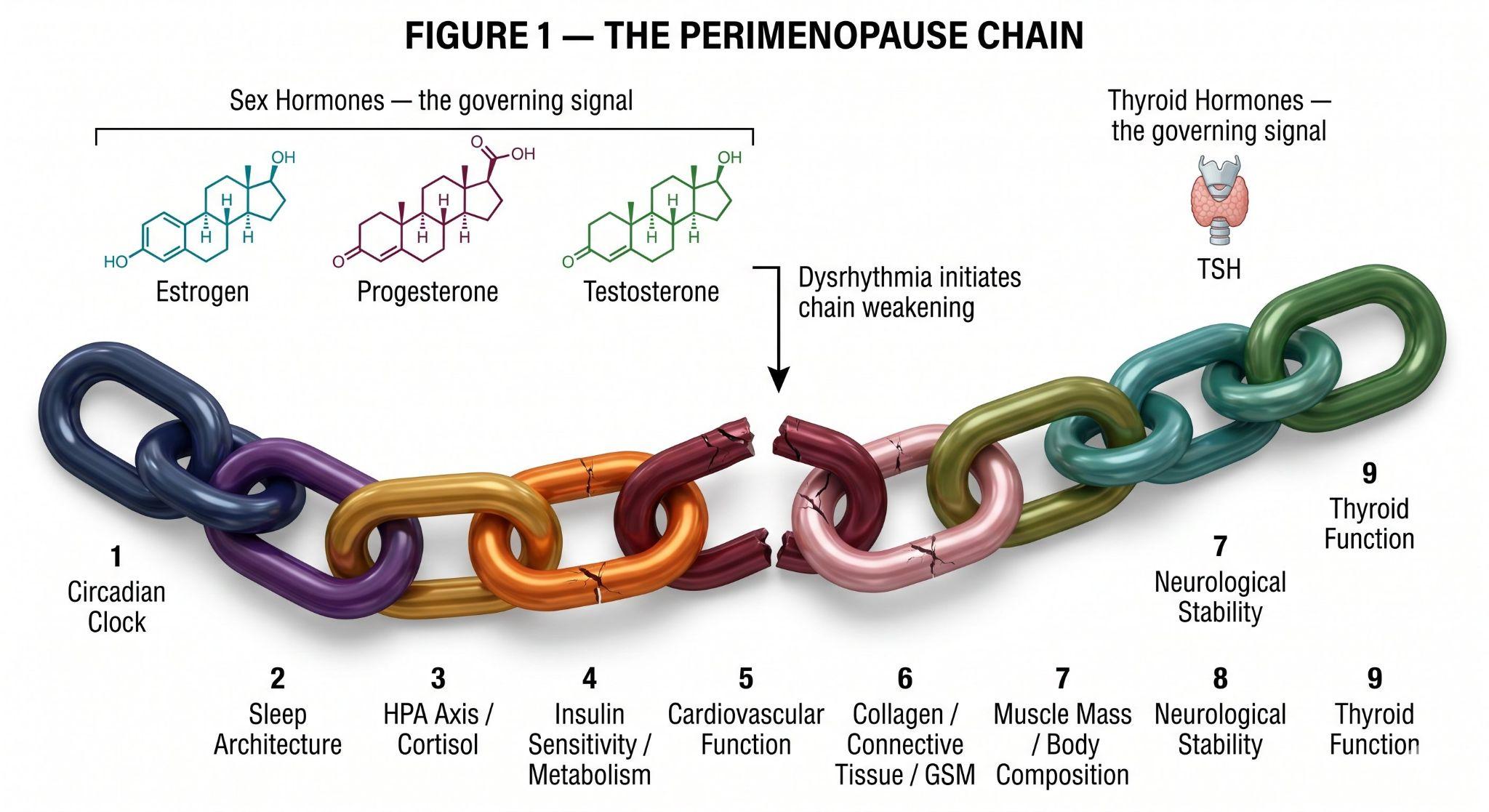
Estrogen receptors in the SCN modulate CLOCK, BMAL1, PER, CRY. As estrogen becomes erratic, circadian amplitude progressively flattens. The first and most consequential link — its weakening propagates through all eight below.
Progesterone decline removes GABA-A night support; flattened circadian amplitude delays melatonin onset. SWS disruption propagates through every remaining chain link. Sleep restoration is the biological prerequisite for everything else working.
The cortisol awakening response (CAR) progressively flattens. Evening cortisol fails to reach its nadir — creating a self-reinforcing loop with Link 2. Morning exhaustion combined with late-night wakefulness is a partially inverted biological clock, driven hormonally.
Three mechanisms compound: estrogen supports insulin receptor tyrosine kinase activity; magnesium homeostasis requires estrogen; estrogen modulates GLP-1 secretion. Body composition shifts occur even with unchanged diet and exercise.
Estrogen maintains endothelial function, arterial elasticity, favourable lipid profiles, and anti-inflammatory vascular tone. The perimenopausal period is the cardiovascular risk inflection point for women. Lp(a) clinical expression amplifies as estrogen cardioprotection withdraws.
Estrogen directly stimulates fibroblast proliferation and collagen gene transcription. Skin collagen 30%+ in the first five years after the final menstrual period. GSM is progressive — it does not improve spontaneously without intervention. Local estrogen or prasterone is the primary evidence-based response.
Estrogen supports satellite cells, suppresses myostatin, supports Type II fibre function, and modulates IGF-1. Its decline raises the anabolic training threshold and extends recovery. Testosterone HRT is the primary pharmacological body composition intervention.
Estrogen is neuroprotective — supporting neurotransmitter synthesis, neuronal plasticity, and glymphatic clearance. Allopregnanolone (from progesterone) is the primary endogenous GABA-A modulator. Its decline creates neurosteroid withdrawal syndrome: anxiety, cognitive impairment, emotional volatility.
Thyroid dysfunction is significantly more prevalent in perimenopausal women and remains systematically underdiagnosed. The bidirectional estrogen-thyroid relationship is clinically critical. Both governing signals must be assessed and interpreted together.
Perimenopause does not arrive into a biologically pristine system. For the majority of women in their 40s, it arrives into a body that has been running on a dysrhythmic biological clock for years — sometimes decades. Social jet lag affects an estimated 60–80% of the working population. Chronic HPA axis activation from professional and personal stress is near-universal in the demographic entering perimenopause.
A woman who enters perimenopause with a pre-existing circadian deficit does not start the transition with nine healthy chain links. She starts with Link 1 already compromised — and the hormonal dysrhythmia of perimenopause compounds that pre-existing damage rather than causing it from scratch. This is why some women deteriorate rapidly at the perimenopausal transition while others with comparable hormonal changes remain functional. The circadian baseline determines the buffer.
Burnout — characterised by exhaustion, cognitive impairment, emotional blunting, and HPA axis dysregulation — is mechanistically identical to several perimenopausal chain disruptions. The flattened cortisol awakening response. The inverted diurnal cortisol pattern. The disrupted sleep architecture. In a woman who has experienced burnout in her 30s or early 40s, the HPA axis arrives at perimenopause already dysregulated.
The clinical consequence: these women respond less completely to HRT alone because the circadian infrastructure HRT needs to work through is itself damaged. They require active circadian rehabilitation — not just hormonal replacement.
- Consistent wake time: The single most powerful circadian anchor available. Even one night of variable wake time degrades circadian amplitude measurably.
- Morning bright light (10–30 minutes): Suppresses melatonin precisely, anchors the SCN to the solar day, sets the phase for the entire 24-hour hormonal cascade.
- Darkness after sunset: Screens, LED lighting, and indoor illumination after 20:00 chronically suppress melatonin onset and delay circadian phase. This is not a lifestyle preference — it is a biological disruption.
- Meal timing consistency: Peripheral clocks in every metabolic organ are entrained by meal timing. Variable meal times independently desynchronise peripheral clocks from the SCN.
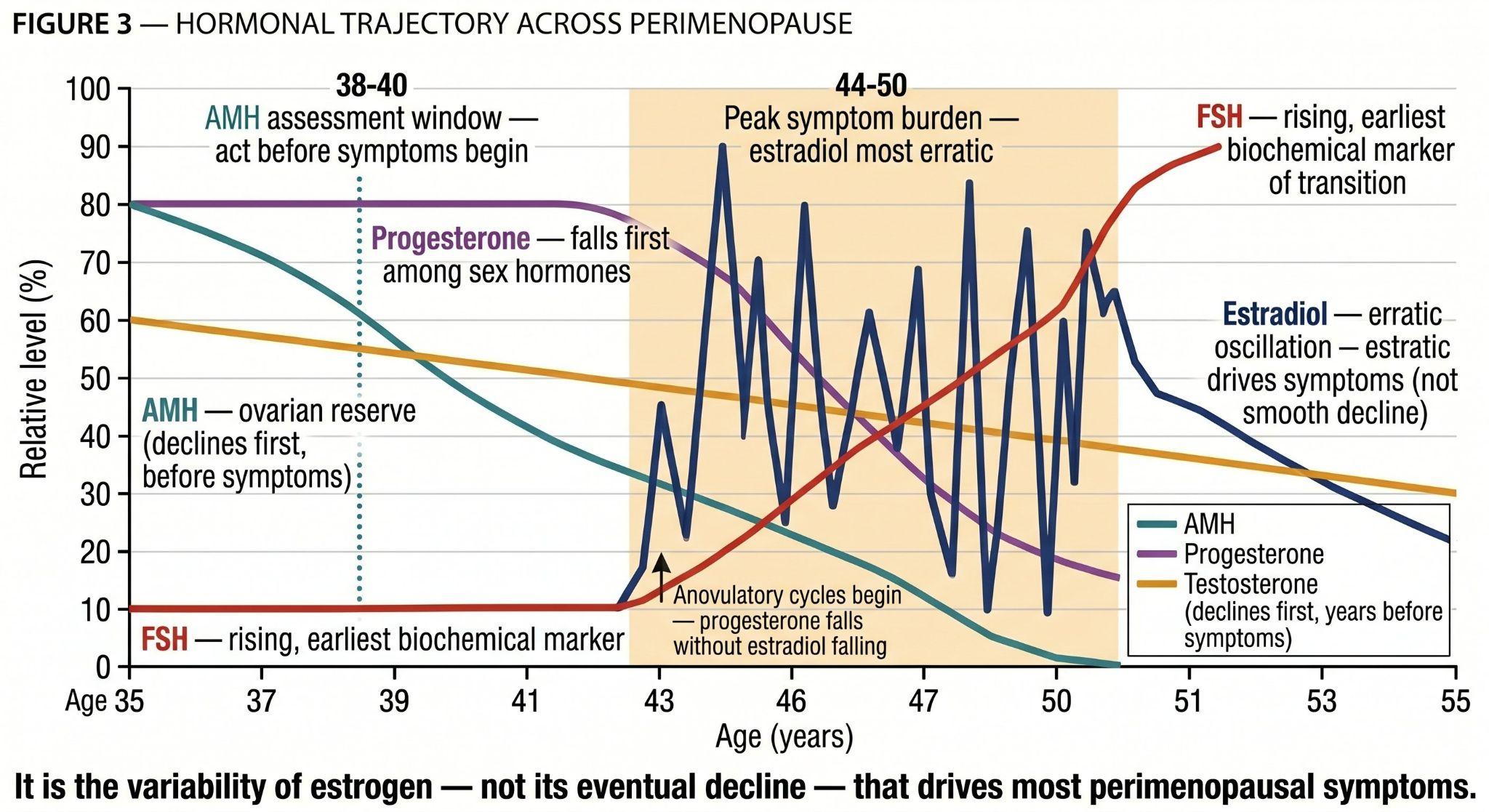
Estrogen is a systemic signalling molecule with receptors in virtually every tissue. Its perimenopause behaviour is an erratic oscillation — supraphysiological peaks alongside precipitous troughs within the same menstrual cycle. This variability, not the eventual decline, drives most perimenopausal symptoms.
Progesterone declines first — typically beginning with anovulatory cycles in the mid-to-late forties — initiating sleep fragmentation and neurological instability before estrogen shows significant change. Testosterone declines gradually, contributing to reduced libido, fatigue, impaired muscle protein synthesis, and diminished motivation.
Anti-Müllerian hormone (AMH), produced by ovarian granulosa cells, reflects the remaining ovarian follicle pool. It begins declining in the late 20s and accelerates through the 30s and 40s — reaching clinically significant levels years before any clinical or hormonal sign of perimenopause is detectable. AMH is the earliest available marker of ovarian aging. A woman with low-normal AMH at age 38 is not perimenopausal — but she is in a strategic planning window.
Thyroid symptom profile overlaps completely with sex hormone deficiency — the primary diagnostic trap. Hypothyroidism increases SHBG, reducing free estradiol and testosterone bioavailability even when total levels appear adequate. Oral estrogen HRT increases TBG, potentially reducing free thyroid hormone in women on thyroid medication. Both governing signals must be assessed and interpreted together — always.
| Life stage | Clinical picture | Primary priority |
|---|---|---|
| Late 30s – early 40s | AMH declining, cycles regular, symptoms subtle or absent. Proactive window. | Establish biological baseline. Circadian health audit. |
| Mid 40s | Anovulatory cycles beginning. Progesterone the first to fall. Sleep fragmentation, anxiety, mood instability. | Micronised progesterone discussion. Day 21 dual testing. |
| Late 40s | Estradiol oscillation maximal — highest symptom burden. Multiple chain links under simultaneous stress. | Full HRT triad conversation. Full laboratory assessment. EscapeMed 30D as chronobiological infrastructure layer. |
| Early 50s | FSH sustained elevation, estradiol declining more consistently. Cardiovascular risk escalating. | HRT continuation essential for eligible women. Bone density monitoring. |
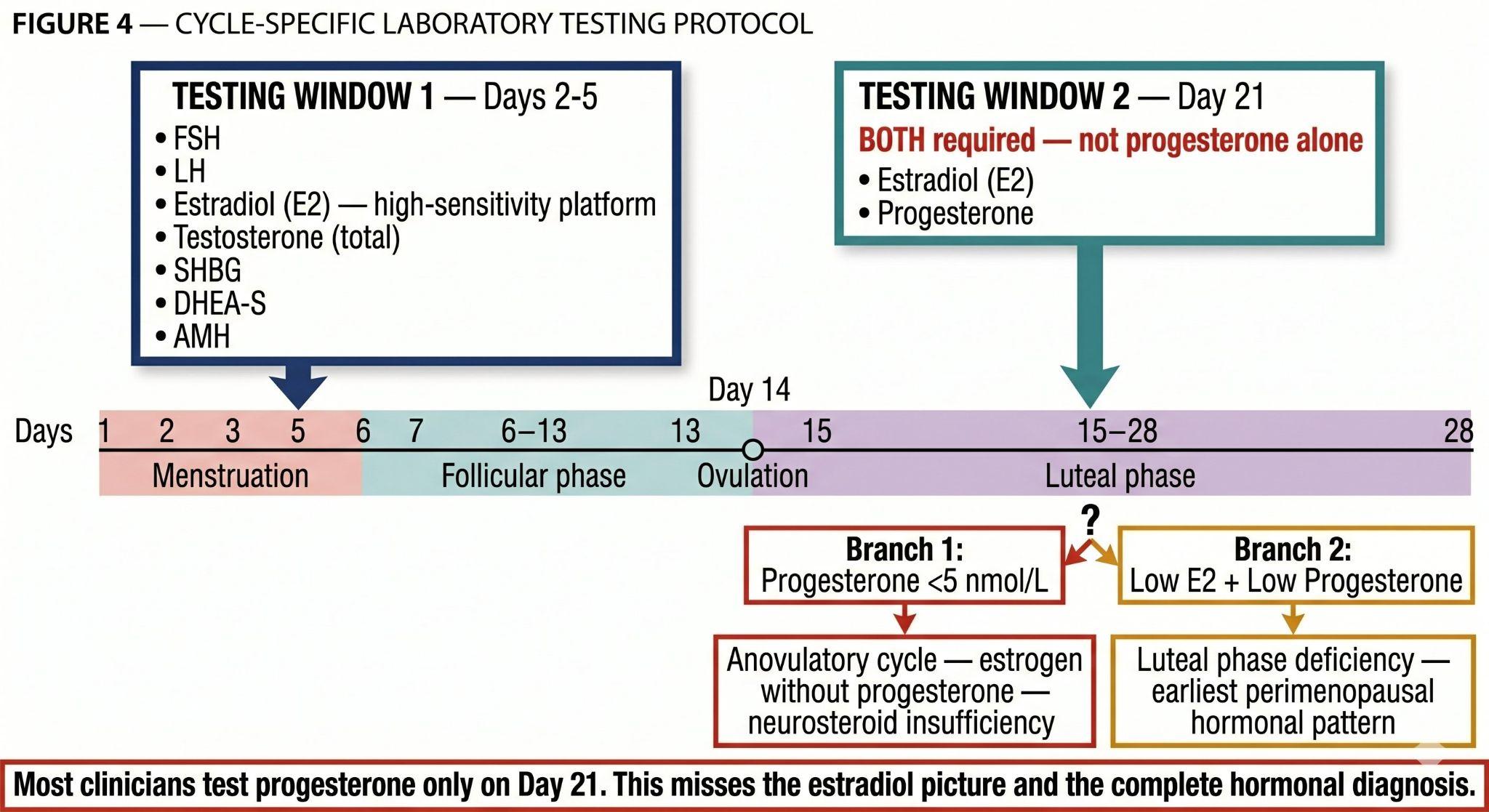
Women with regular cycles — two timepoints required: Days 2–5 (FSH, LH, estradiol, testosterone, SHBG, DHEA-S, AMH) and Day 21 (BOTH estradiol AND progesterone simultaneously). Progesterone below 5 nmol/L indicates anovulatory cycle. Most clinicians test progesterone only on Day 21 — this misses the complete picture.
Analytical platform: High-sensitivity platforms (Roche Elecsys and equivalent) are mandatory for perimenopausal sex hormone measurement. Standard immunoassays lose precision below 100 pmol/L — precisely the range most clinically relevant in perimenopause. Do not compare values across different platforms or laboratories.
The following table consolidates 29 clinical parameters with their standard laboratory ranges and optimal perimenopausal targets. The gap between these two columns represents one of the most consistent sources of undertreated perimenopause: results that are "normal" by laboratory criteria but significantly suboptimal for perimenopausal biology.
| Parameter | Standard range | Optimal perimenopausal target | Clinical notes |
|---|---|---|---|
| BMI | 18.5–24.9 kg/m² | Perimenopausal caveat: poor body composition marker | Normal BMI with elevated visceral fat is common. Waist <80cm and DEXA more informative. BMI ≥30: transdermal HRT mandatory. |
| TSH | 0.5–4.5 mIU/L | Optimal: 1.0–2.5 mIU/L | Values 2.5–4.5 mIU/L may be suboptimal despite being "normal". Symptom profile indistinguishable from estrogen deficiency. |
| Free T3 | 3.5–6.5 pmol/L | >4.5 pmol/L preferred | Low-normal T3 with normal TSH suggests impaired T4-T3 conversion — common with chronic HPA stress. |
| Free T4 | 9–19 pmol/L | Mid-to-upper range preferred | Oral estrogen HRT increases TBG, potentially reducing free T4. Recheck at 3 months after oral HRT. Transdermal avoids this. |
| Anti-TPO antibodies | <34 IU/mL | Screen once at baseline | Hashimoto's thyroiditis peaks in perimenopause. Positive result changes monitoring frequency. |
| Estradiol (E2) | Highly variable | Symptom-guided; 200–400 pmol/L on HRT | High-sensitivity platform mandatory. Do not compare across labs. On HRT: test minimum 4 hours after patch/gel application. |
| FSH | Menopausal: >25 IU/L | Context-dependent | Rising FSH is a useful perimenopausal marker but should not be used in isolation to diagnose or exclude perimenopause. |
| Progesterone (Day 21) | >16 nmol/L = ovulatory | >16 nmol/L confirms ovulation; <5 nmol/L = anovulatory | Test SIMULTANEOUSLY with Day 21 estradiol. On oral micronised progesterone: serum P is NOT a reliable monitoring endpoint — see critical note below. |
| Total testosterone | 0.3–2.4 nmol/L | Free T (calculated from total T + SHBG) is the clinically relevant value | Total T without SHBG is clinically incomplete. Test morning. |
| SHBG | 16–120 nmol/L | Monitor change from baseline | Oral estrogen significantly increases SHBG. Transdermal does not. High SHBG reduces free sex hormone bioavailability. |
| DHEA-S | Age-dependent | Above lower quartile for decade of life | Declines with age and chronic HPA stress. |
| AMH | Age-dependent | Low-normal for age in late 30s = proactive window | Earliest available marker of ovarian aging. Strategic planning tool. Include in baseline panel for any woman over 35. |
| HOMA-IR | Not routinely reported | Target <2.0; concern >2.0; significant >2.5 | Calculated: (fasting insulin mU/L × fasting glucose mmol/L) ÷ 22.5. |
| Fasting insulin | <25 mU/L | Optimal: <10 mU/L | Values 10–25 mU/L with normal glucose indicate compensated insulin resistance. |
| Fasting glucose | 3.9–6.1 mmol/L | Optimal: <5.0 mmol/L | Standard range accepts values that indicate developing metabolic dysfunction. |
| HbA1c | <48 mmol/mol (<6.5%) | Optimal: <39 mmol/mol (<5.7%) | Standard threshold misses the prediabetic range where intervention is most effective. |
| Lp(a) | <75 nmol/L or <30 mg/dL | Elevated risk: >125 nmol/L | Genetically determined but clinically expressed with greater impact as estrogen withdraws. Test once. |
| hs-CRP | <5 mg/L | Cardiovascular risk: <1 low; 1–3 moderate; >3 high mg/L | HPA dysrhythmia and sleep fragmentation both drive elevated hs-CRP. |
| ApoB | <130 mg/dL | Optimal: <90 mg/dL | More accurate cardiovascular risk marker than LDL. |
| Homocysteine | <15 µmol/L | Optimal: <10 µmol/L | Responds to B6, B12, folate. Independent cardiovascular and cognitive risk factor. |
| Ferritin | 12–300 µg/L | Functional optimum: >50 µg/L | Heavy perimenopausal bleeding causes iron deficiency presenting identically to hormonal symptoms. One of the most commonly missed diagnoses. |
| Vitamin B12 | 150–700 pmol/L | Optimal: >300 pmol/L | Neurological symptoms of B12 deficiency are indistinguishable from perimenopausal neurological disruption. |
| 25-OH Vitamin D | >50 nmol/L | Optimal: 100–150 nmol/L | Standard threshold prevents rickets — does not optimise the functions relevant in perimenopause. Most Europeans need 2,000–4,000 IU/day. |
| Omega-3 Index | Not on standard panels | Target: >8% EPA+DHA | Most Europeans test 4–6%. Below 8% associated with increased cardiovascular, neurological, and inflammatory risk. |
| Prolactin | <500 mIU/L | Screen once at baseline | Elevated prolactin mimics perimenopausal symptoms. One-time baseline screen. |
| Blood pressure | <140/90 mmHg | Optimal: <120/80 mmHg home monitoring | Consistent home readings >135/85 mmHg warrant clinical attention. New-onset hypertension in perimenopause is frequently hormonal. |
| Waist circumference | No standard on lab forms | Target: <80 cm (European women) | Most accessible visceral adiposity marker. Waist-to-height ratio <0.5 is more predictive. |
Clinical reference tool, not a prescription. Values should be interpreted in clinical context by a qualified physician.
Serum progesterone is NOT a reliable monitoring endpoint for oral micronised progesterone therapy. Oral micronised progesterone undergoes first-pass hepatic metabolism to allopregnanolone — which does NOT appear as progesterone in serum. A low serum P on micronised progesterone does NOT indicate underdosing. The clinical endpoint is symptom response: sleep quality, anxiety reduction, mood stability. This is one of the most common errors in HRT monitoring worldwide.
| Hormone / marker | Target on HRT | When and how to test | Critical notes |
|---|---|---|---|
| Estradiol (E2) on transdermal HRT | Target: 200–400 pmol/L for symptom control. Some women require 400–600 pmol/L. | Test minimum 4 hours after patch or gel application. High-sensitivity platform. Recheck at 3, 6, 12 months. | If E2 adequate but symptoms persist, check SHBG (high SHBG reduces free E2). Symptom relief is co-primary endpoint. |
| Progesterone on oral micronised progesterone | CRITICAL: Serum progesterone is NOT a reliable monitoring marker. | No serum target applicable for dosing decisions. Clinical endpoint is symptom response. | Oral micronised progesterone metabolises to allopregnanolone — which does NOT appear as serum progesterone. A low serum P does NOT indicate underdosing. |
| Testosterone on HRT | Free testosterone in upper quartile of premenopausal female reference range. Total T: 0.5–2.0 nmol/L. | Test morning. Test 4–6 weeks after initiation. SHBG mandatory alongside total T. Recheck at 3 and 6 months. | Symptom response is co-primary endpoint: libido, energy, cognitive clarity. Total T without SHBG is clinically incomplete. |
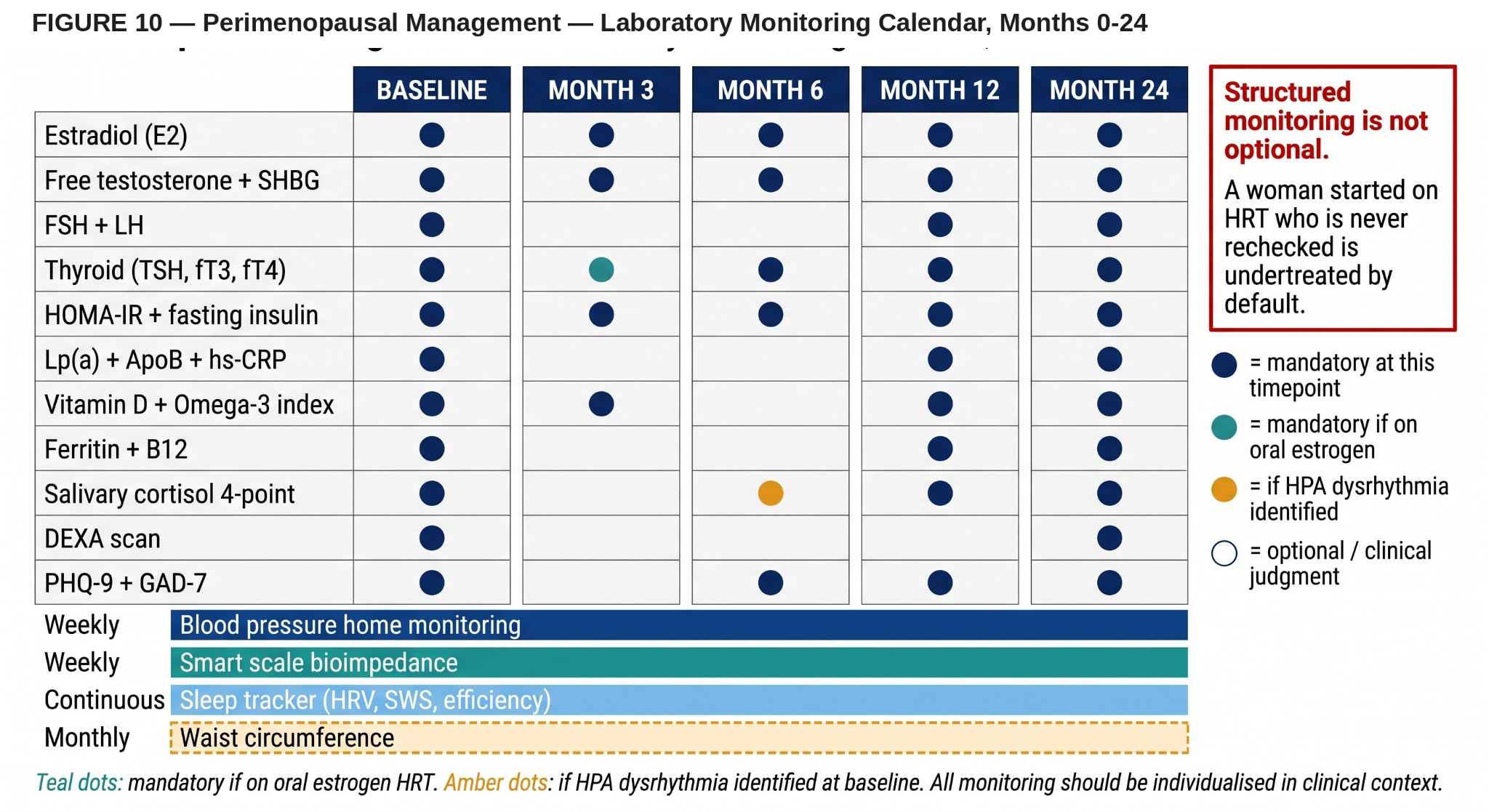
| Post-HRT monitoring schedule | 3 months: E2, free T, SHBG, symptom assessment. 6 months: full panel, HOMA-IR. 12 months: comprehensive review. Annually thereafter. | Structured monitoring is not optional. | The most common HRT management failure is not the prescription — it is the absence of structured follow-up. A woman never rechecked is undertreated by default. |
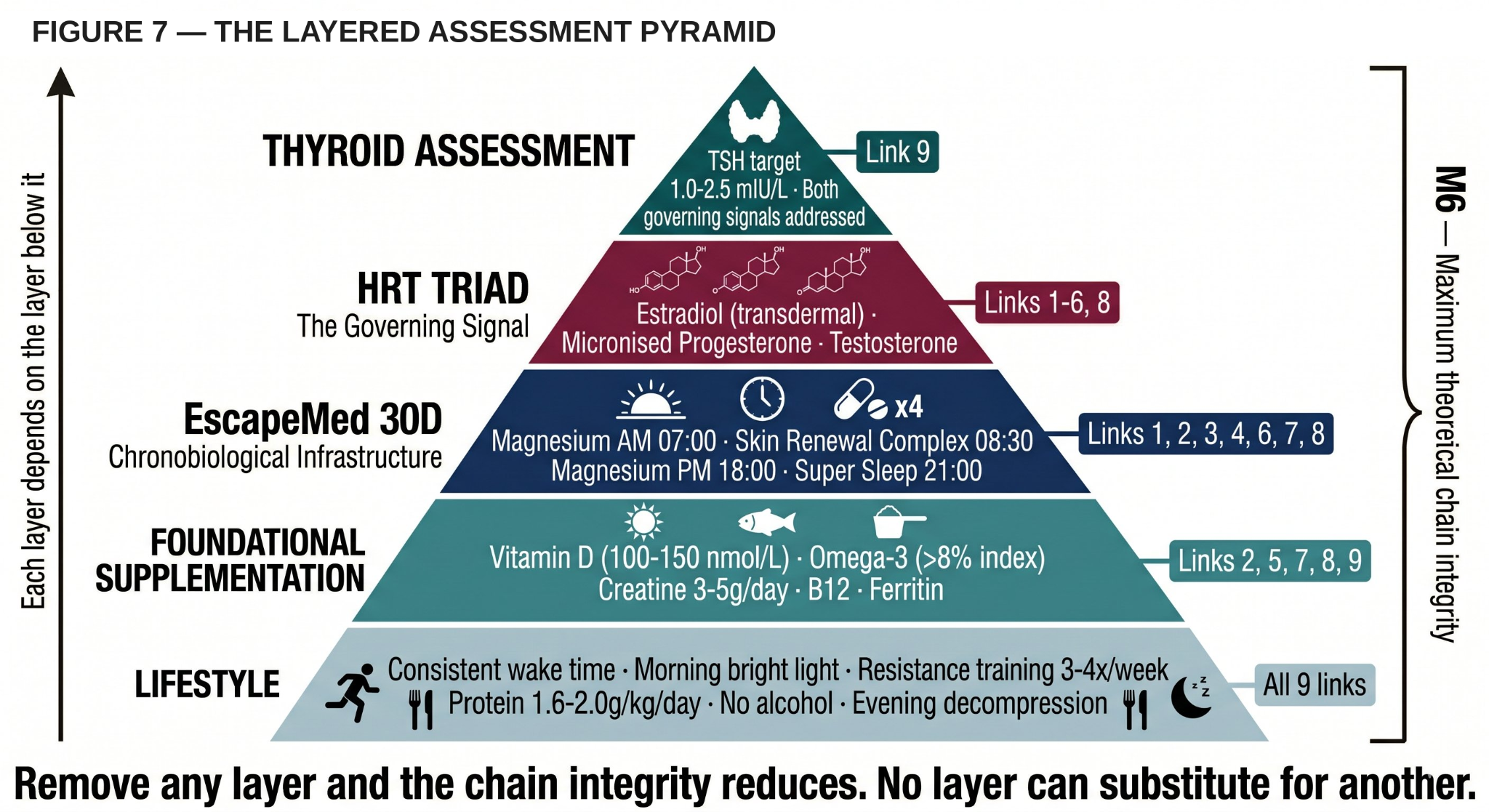
No single intervention addresses all nine chain links. Four categories, different mechanisms, different chain levels. Greatest value in coordinated combination.
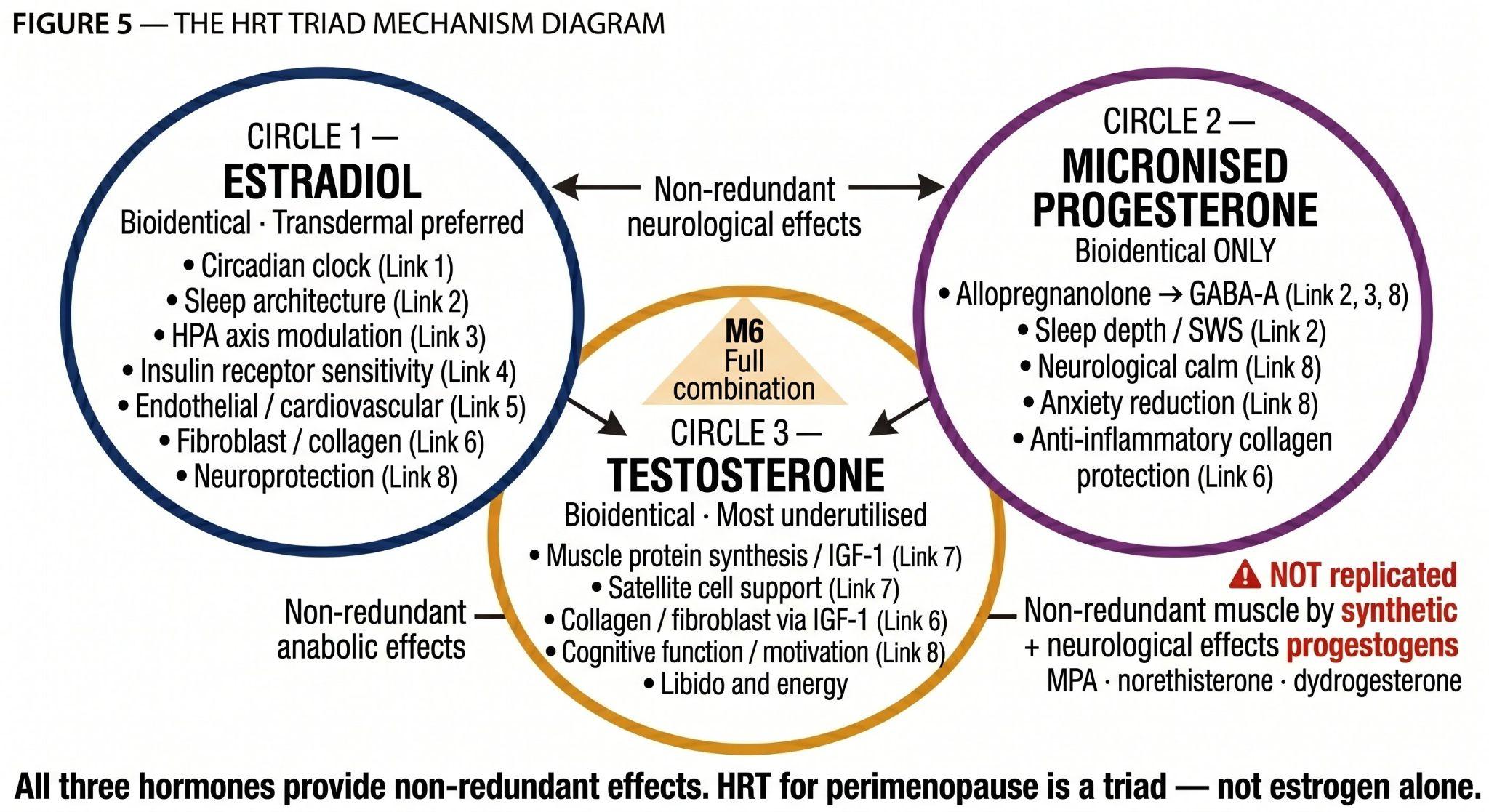
HRT is the only intervention that addresses the governing signal directly. No dietary supplement, no lifestyle programme restores estrogen. Modern HRT for perimenopause must be understood as a triad — each hormone has distinct, non-redundant biological effects.
- Estradiol (bioidentical, transdermal preferred): The primary governing signal. Addresses Links 1–6 and 8 directly. Transdermal delivery avoids first-pass hepatic metabolism, does not increase TBG, and does not carry the venous thromboembolism risk of oral estrogen.
- Micronised progesterone (bioidentical — NOT synthetic progestogen): Metabolised to allopregnanolone — the endogenous GABA-A positive allosteric modulator responsible for neurological calm, sleep depth, and anxiety regulation. This neurological action is NOT shared by synthetic progestogens (medroxyprogesterone acetate, norethisterone, dydrogesterone). Prescribing a synthetic progestogen while expecting the neurological benefits of progesterone is a clinical mismatch that leaves women undertreated at Link 8.
- Testosterone (bioidentical): The most consistently underutilised component. Supports libido, muscle protein synthesis via IGF-1, cognitive function, motivation, and energy. Should be assessed in every perimenopausal woman — not only those presenting with low libido.
The fear of HRT in public consciousness is based on the WHI trial, which used synthetic progestogens and conjugated equine estrogen — not bioidentical hormones. The increased breast cancer risk in that trial was approximately +0.1% per year of combined HRT use — of the same order of magnitude as 1–2 units of alcohol daily or sedentary lifestyle, risks rarely discussed with equal urgency. The absolute cardiovascular, bone, and cognitive risks of untreated perimenopause in eligible women are substantially larger. HRT initiated before age 60 or within 10 years of the final menstrual period provides cardiovascular protection, reduces all-cause mortality, and protects bone.
"The fear of HRT that persists in public consciousness is costing women years of preventable suffering. The pharmacology that created that fear is not the pharmacology used in modern bioidentical therapy. These must not be conflated."
- Sleep timing: Consistent wake time — the single most powerful circadian anchor. Morning bright light. Darkness after sunset. Bedroom 18°C.
- Nutrition: Protein 1.6–2.0g/kg/day distributed across meals. Anti-inflammatory pattern. Carbohydrates front-loaded to morning. No eating within 3 hours of sleep.
- Training: Resistance training minimum 3×/week with progressive overload. Morning preferred for circadian reinforcement.
- Alcohol: Suppresses REM and SWS directly; worsens hot flushes; impairs hepatic estrogen metabolism; increases breast cancer risk. Minimisation is a clinical recommendation.
- Vitamin D: Target 100–150 nmol/L. 2,000–4,000 IU/day. Links 5, 8, 9.
- Omega-3 (EPA + DHA): Target Omega-3 Index >8%. 2–3g EPA+DHA/day. Links 2, 5, 8. Most Europeans test 4–6%.
- Creatine: 3–5g/day standalone powder. Evidence for muscle preservation (Link 7) and cognitive function (Link 8) in perimenopausal women.
The biological mechanisms of dietary supplements do not change in perimenopause. What changes is the biological context — the specific deficits that perimenopause creates — under which those mechanisms become most needed. Perimenopause creates: functional magnesium insufficiency; declining GABAergic tone; flattened circadian amplitude; accelerating collagen loss; disrupted insulin signalling; and reduced GLP-1 response. Under these conditions, timed delivery of specific nutritional mechanisms at the correct circadian phase amplifies their effect.
"The gap between what supplements could do and what they actually produce is not a gap in ingredient quality. It is a gap in timing, architecture, and the correct diagnosis of the underlying problem. Supplements that ignore timing cannot address a timing problem."
— Samarin, 2026The EscapeMed 30D system is a four-formula, 30-ingredient chronobiological supplement architecture delivering phase-specific biological support at four timed moments across the 24-hour cycle. It is the chronobiological supplementation layer of the M6 intervention framework — supporting biological infrastructure without claiming to restore the hormonal governing signal.
| Formula | Timing | Primary mechanisms | Chain links | Perimenopausal relevance |
|---|---|---|---|---|
| Magnesium AM (7 ingredients) | 07:00–09:00 with breakfast | 5 magnesium salt forms: malate + succinate (TCA cycle substrates), bisglycinate (repletion), L-ascorbate (catecholamine + collagen cofactor), citrate. B6-P5P. Inositol (serotonin receptor sensitisation). | Links 1, 3, 4, 8 | Estrogen decline flattens the cortisol awakening response and disrupts magnesium homeostasis through renal reabsorption. Supports morning bioenergetic activation at the precise moment perimenopause most compromises. |
| Skin Renewal Complex (14 ingredients) | 08:30–11:00 late morning | Complete 10-step collagen synthesis cofactor chain: vitamin C, zinc, copper, silicon, MSM, glycine. 6-compound antioxidant and MMP-inhibition system. Hyaluronic acid ECM hydration. CoQ10 for fibroblast mitochondrial support. | Links 1, 5, 6 | Estrogen-dependent fibroblast stimulation declines — the fibroblast window persists. Cofactor delivery at this precise circadian moment determines collagen synthetic output. |
| Magnesium PM (6 ingredients) | 18:00–20:00 with dinner | 3 PM-exclusive salts: taurate (extrasynaptic GABA-A in thalamus), lactate (Cori cycle nocturnal glycogen), gluconate (NADPH for nocturnal glutathione). CLOCK/BMAL1 support. NMDA modulation. | Links 1, 3, 4, 7, 8 | As estrogen and progesterone decline the evening biological transition becomes imprecise. Supports the transition sex hormones previously orchestrated. |
| Super Sleep (8 ingredients) | 21:00–22:00 before sleep | Melatonin microdose 0.1–0.2mg (SCN darkness signal). 4 convergent GABA-A pathways (theanine, apigenin, taurine, bisglycinate). Glycine (SWS + core temperature). Ashwagandha KSM-66 (HPA normalisation). L-Tryptophan + B6-P5P. | Links 1, 2, 3, 8 | Progesterone withdrawal removes the GABA-A neurochemical night signal. Super Sleep addresses each disrupted neurobiological mechanism through independent non-hormonal pathways. |
What EscapeMed 30D does not include: Omega-3 and vitamin D (individually calibrated standalone supplementation required). Creatine (dose-volume incompatible with capsule format). These are deliberate design decisions.
All mechanisms theoretical — based on ingredient-level physiology, not controlled trials in perimenopausal populations. EscapeMed 30D is a food supplement (EU Directive 2002/46/EC) and cannot claim to treat, prevent, or cure any condition.
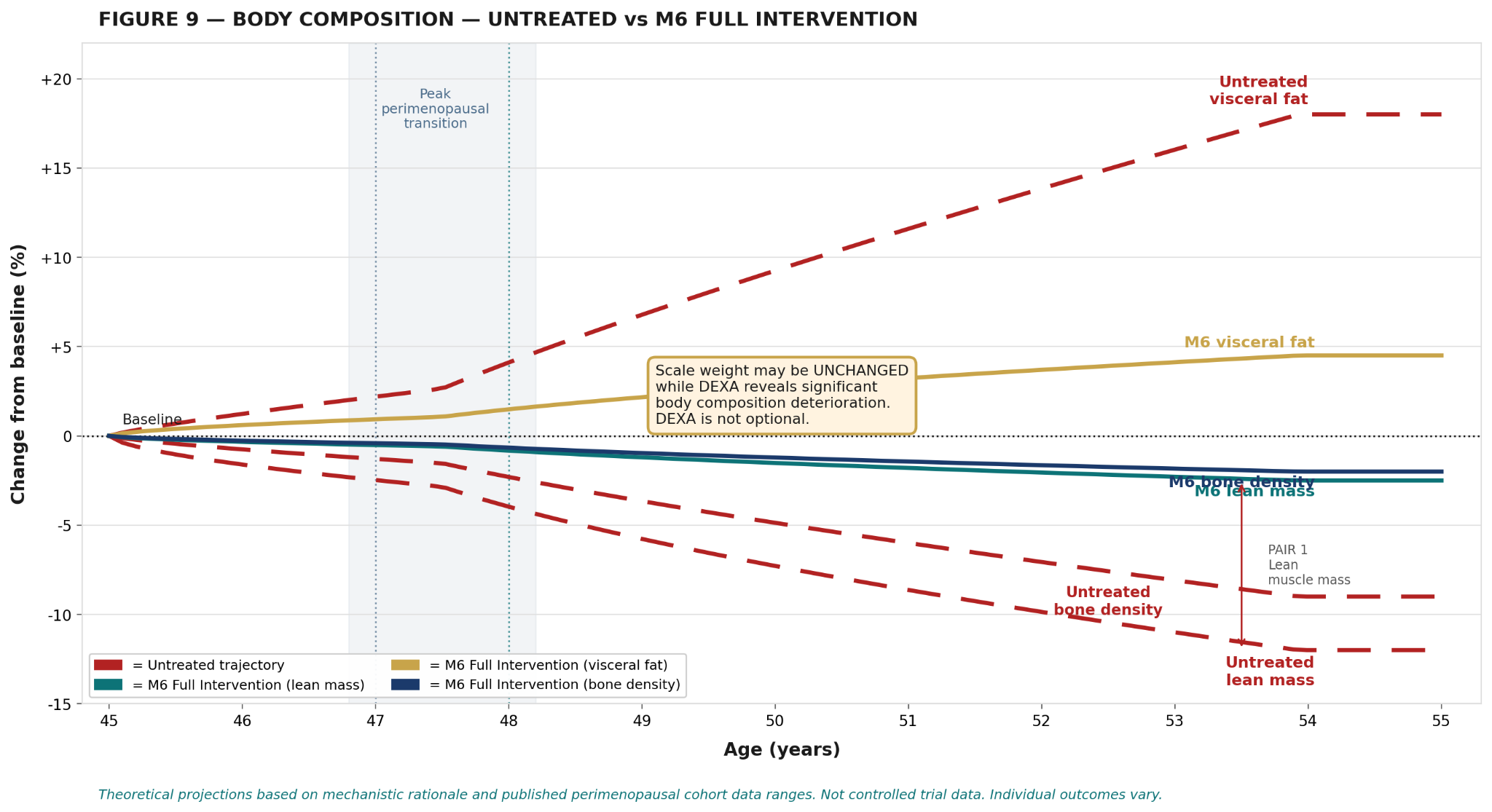
Obesity amplifies virtually every chain link simultaneously. Visceral fat in perimenopause is estrogenically active through peripheral aromatisation — producing estrogen metabolites that worsen hormonal imbalance rather than compensate for it. Transdermal estradiol is mandatory in obese perimenopausal women — oral estrogen doubles VTE risk in obesity. GLP-1 receptor agonists become the most clinically relevant pharmacological adjunct. DEXA — not BMI — is essential.
Bioidentical estradiol HRT actually improves insulin sensitivity in this population — it is not contraindicated in metabolic disease. HOMA-IR should be monitored quarterly. The combination of lifestyle, HRT, and GLP-1 receptor agonist where indicated represents the most complete framework.
Transdermal estradiol — not oral — is mandatory. Lp(a) elevation with existing cardiovascular disease requires specialist assessment including carotid intima-media thickness ultrasound. New-onset hypertension in perimenopause is frequently hormonal — hormonal assessment before antihypertensive initiation is warranted.
The critical clinical question before initiating antidepressants in a perimenopausal woman: has she been assessed for estrogen and progesterone status? Has micronised progesterone been considered for the allopregnanolone/GABA-A component? In many cases, appropriate HRT significantly changes the neurobiological picture. HRT and psychiatric treatment are complementary — but the hormonal assessment must come first.
OSA prevalence increases significantly in perimenopause — driven by reduced progesterone's protective effect on upper airway muscle tone. A woman with severe sleep fragmentation unresponsive to HRT and Super Sleep protocol should be screened for OSA before concluding the intervention is insufficient. Untreated OSA renders every sleep intervention partially ineffective.
Six theoretical frameworks comparing expected chain outcomes at 12 months. Subject: 47-year-old perimenopausal woman, symptomatic, normal thyroid, BMI 24, moderately active, no comorbidities. Theoretical constructs grounded in mechanistic rationale — not controlled trial evidence.
Progressive chain weakening across all nine links. The biological cost of unaddressed perimenopause. Muscle loss, cardiovascular risk escalation, bone loss, neurological deterioration, and metabolic dysfunction continue unchecked.
Partial circadian stabilisation. Sleep efficiency improves but SWS not restored without progesterone support. Insulin sensitivity attenuation. Chain weakening slows but continues. Meaningful for Link 7 (muscle) and Link 4 (metabolism).
Four daily Zeitgeber anchors reinforce the weakening circadian rhythm. Sleep architecture supported through GABAergic and melatonergic pathways. Governing signal not restored — biological infrastructure supported through available mechanisms. Best response in Links 1, 2, 6.
Governing signal restored. Progressive repair across Links 1–6, 8. Muscle mass remains training-and-protein-dependent. Collagen synthesis below restored potential without cofactor delivery at the biological window. HRT opens the biological doors — lifestyle and supplementation determine what walks through them.
Additive Zeitgeber reinforcement — behavioural and molecular. Optimal for women not eligible for HRT or in early perimenopausal stages. Meaningful improvement across Links 1–4 and 6–7. Governing signal not restored.
All layers coordinated. HRT restores the governing signal. Lifestyle provides the foundation and Zeitgeber inputs. EscapeMed 30D provides molecular cofactors and timing. Foundational supplementation addresses gaps. Thyroid assessed and treated. All nine links addressed. Maximum theoretical chain integrity.
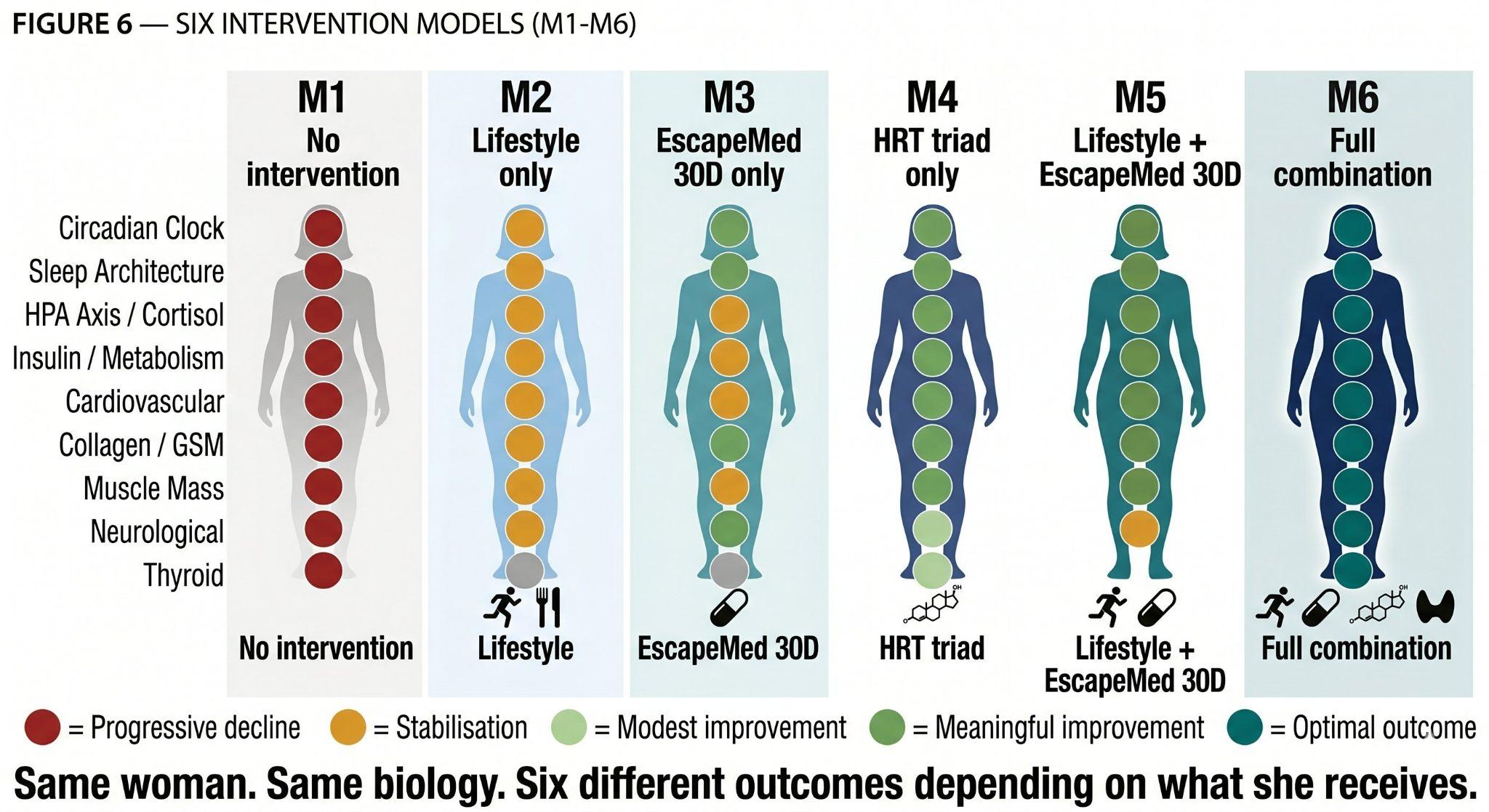
| Chain Link | M1 None | M2 Lifestyle | M3 EscapeMed | M4 HRT | M5 L+EM | M6 Full |
|---|---|---|---|---|---|---|
| 1. Circadian Clock | ↓↓ | ↑ | ↑↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 2. Sleep Architecture | ↓↓ | ↑ | ↑↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 3. HPA Axis / Cortisol | ↓↓ | ↑ | ↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 4. Insulin / Metabolism | ↓↓ | ↑ | ↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 5. Cardiovascular | ↓↓ | ↑ | ↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 6. Collagen / Connective Tissue + GSM | ↓↓ | ↔ | ↑↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 7. Muscle Mass / Body Composition | ↓↓ | ↑↑ | ↑ | ↑↑ | ↑↑↑ | ↑↑↑ |
| 8. Neurological Stability | ↓↓ | ↑ | ↑↑ | ↑↑ | ↑↑ | ↑↑↑ |
| 9. Thyroid Function | ↓ | ↔ | ↔ | ↑ | ↔ | ↑↑+Rx |
All ratings theoretical. ↓↓ progressive decline · ↔ stabilisation · ↑ modest improvement · ↑↑ meaningful improvement · ↑↑↑ maximum theoretical benefit
A 30-day single-arm pilot observational study (N=20 at baseline; N=21 at Day 30 with one late participant entry) provides preliminary hypothesis-generating evidence on the EscapeMed 30D chronobiological supplement system. Presented with full transparency as hypothesis-generating evidence only. No control group.
14 women (70%) and 6 men (30%). Age range 27–61 years (mean 47.2 years). 11 of the 14 women (79% of female participants) were aged 45–54 — the peak perimenopause decade. Baseline burden: 100% reported body NOT in full balance; 90% experienced night wakings; 80% reported HIGH or VERY HIGH psychological stress; only 10% woke rested.
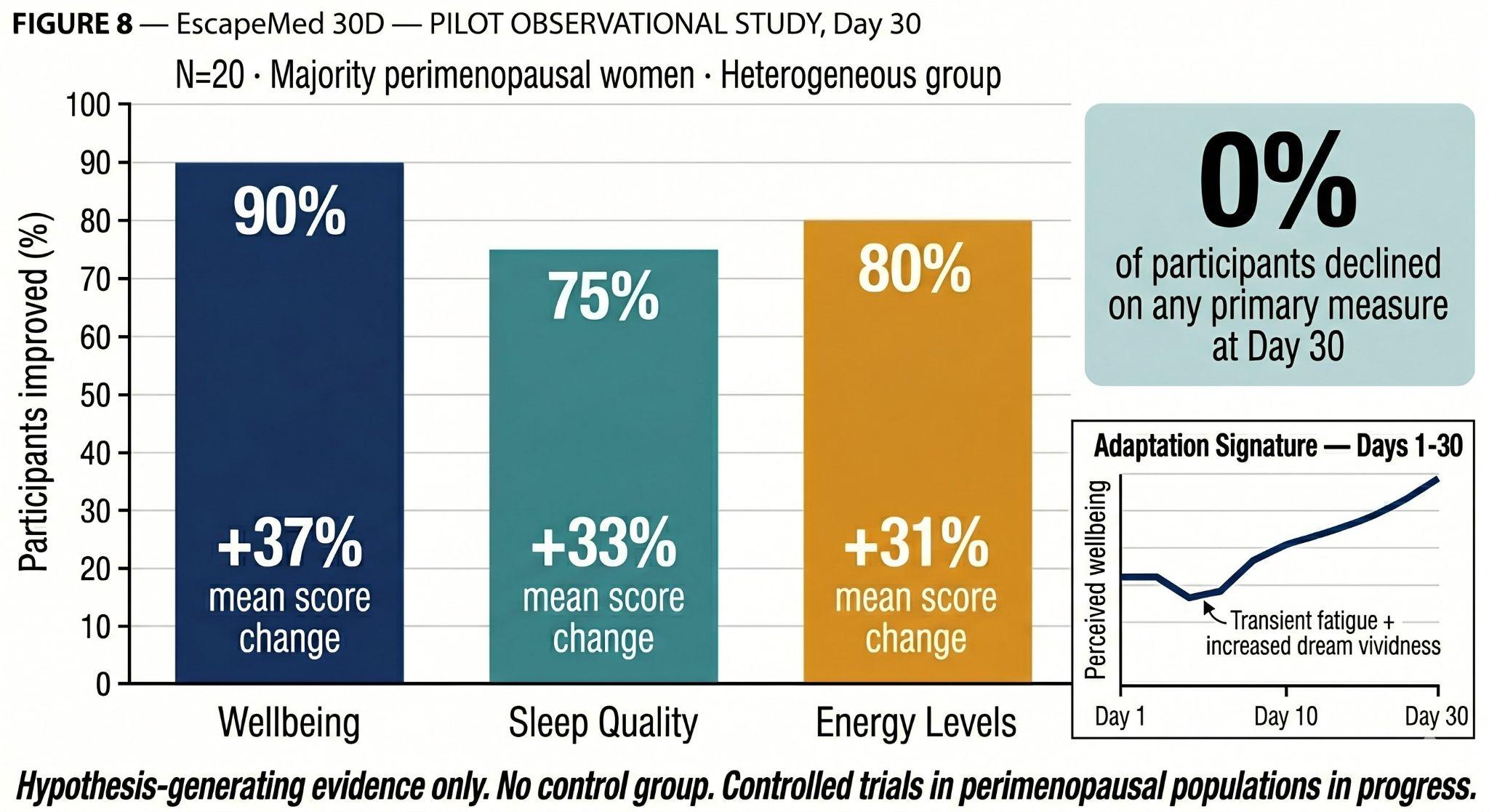
Morning waking quality at Day 30: 38% woke rested (up from 10%); 0% woke tired (down from 35%).
Adaptation Signature (Days 3–5): 50% of participants reported increased dream vividness and transient afternoon fatigue on Days 3–5 — attributed to glycine-driven REM density increase and ashwagandha-mediated HPA normalisation respectively. This pattern is consistent with early circadian resynchronisation.
Single-arm, open-label, self-report observational design with N=20. No control group. Independent replication in a controlled study is required. An ongoing prospective pilot study with a larger perimenopausal cohort, objective sleep assessment, biomarker panel, and biological age measurement is in progress. Results anticipated late 2026.
First: perimenopause is one process. The clinical entry point is the chain — not the symptom list, not the specialist referral, not the hormone level in isolation. Treating it as a collection of independent problems will always produce partial results.
Second: no supplement restores hormones — and this must be communicated clearly, consistently, and without equivocation to every perimenopausal patient. Women who choose supplements over HRT because they were not offered an informed clinical conversation are being failed by the healthcare system.
Third: monitoring is the mechanism by which HRT works properly. A woman started on HRT who is never rechecked is undertreated by default. The progesterone monitoring caveat — serum progesterone is not a reliable endpoint for micronised progesterone therapy — is among the most practically important clinical notes in this review.
Fourth: timing matters more in perimenopause than in any earlier life stage. The circadian amplitude that previously provided robust biological timing signals is weakening. Interventions that reinforce circadian timing produce amplified effects relative to the same interventions delivered without timing awareness.
Fifth: the WHI trial legacy continues to distort perimenopausal prescribing. The WHI trial used synthetic progestogens and conjugated equine estrogen — not bioidentical hormones. Its findings are not transferable to bioidentical HRT.
Three explanations account for the majority of cases:
- The circadian clock was already broken: Years of cortisol dysregulation, chronic stress, and social jet lag compromised Link 1 before perimenopause began. HRT restores estrogen's input to the SCN — but cannot rebuild a clock infrastructure that was already damaged. Active circadian rehabilitation is required alongside hormonal therapy.
- The chain links have structural lag: Collagen rebuilding requires months. Muscle satellite cell reactivation requires progressive training plus adequate SWS plus protein adequacy — simultaneously. Bone density changes over years. The chain links damaged before HRT need active intervention at their specific biological level.
- Labs are normal — but not optimal: Ferritin at 18 µg/L is "within normal range" — but functionally insufficient for energy, cognition, and hair. Vitamin D at 52 nmol/L is "sufficient" — but far below the 100–150 nmol/L where neurological and immune function is optimised. TSH at 3.8 mIU/L is "normal" — but hypothyroid in a meaningful proportion of symptomatic women. Normal is not optimal.
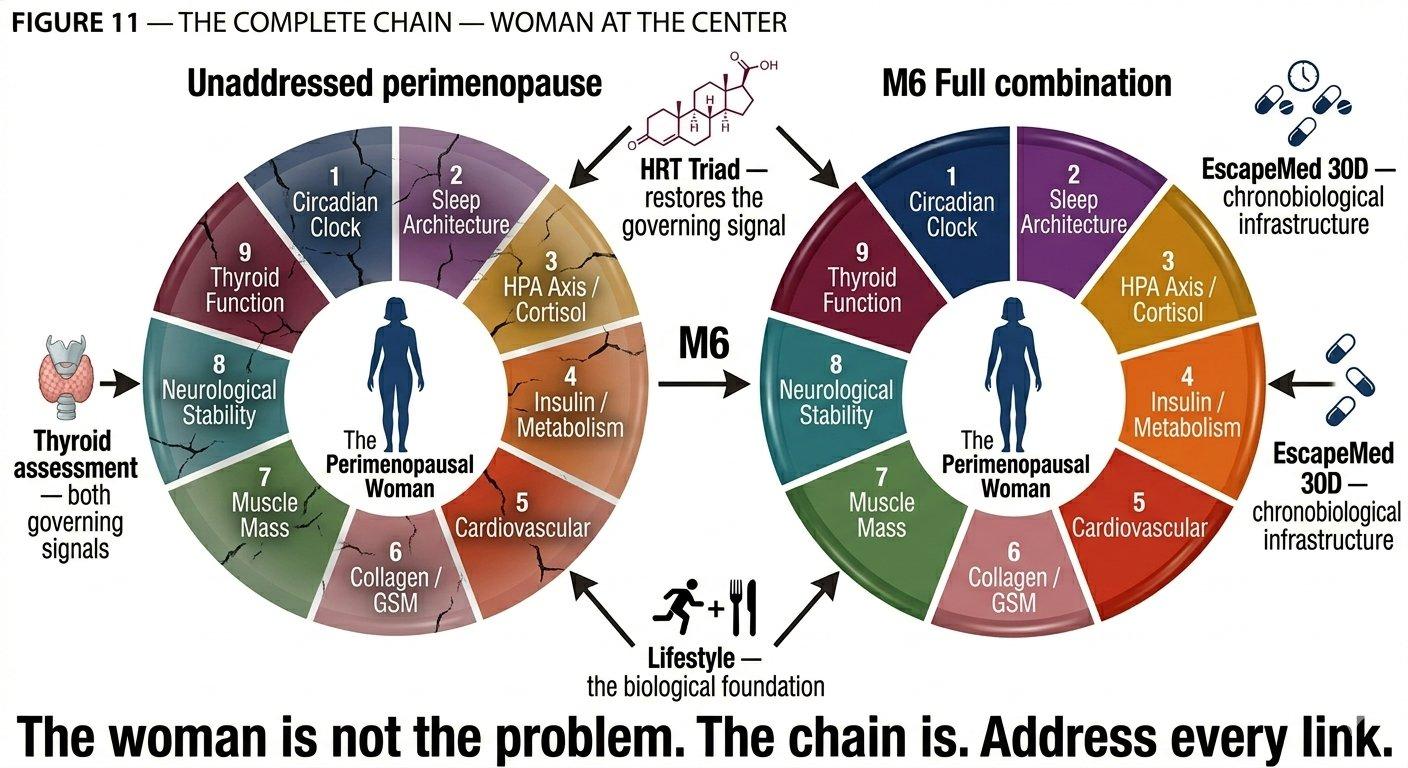
Perimenopause is a chain. Nine biological systems, governed by two master signals — sex hormones and thyroid hormones — whose progressive dysrhythmia initiates cascading disruption. The chain is only as strong as its weakest link. No supplement restores the governing signal. HRT does. The two are not competing alternatives — they are different tools for different levels of the same chain. Monitoring at 3, 6, and 12 months is not optional follow-up. It is the clinical infrastructure that separates effective hormonal management from hormonal neglect.
"You are not falling apart. You are not ageing prematurely. You are experiencing a predictable, biological, mechanism-driven transition — and the symptoms you are experiencing are signals from a chain that is losing coherence, link by link, because its governing signals are becoming erratic. Understanding this matters — not because the biology makes it easier, but because understanding the mechanism gives you tools that symptom lists do not."
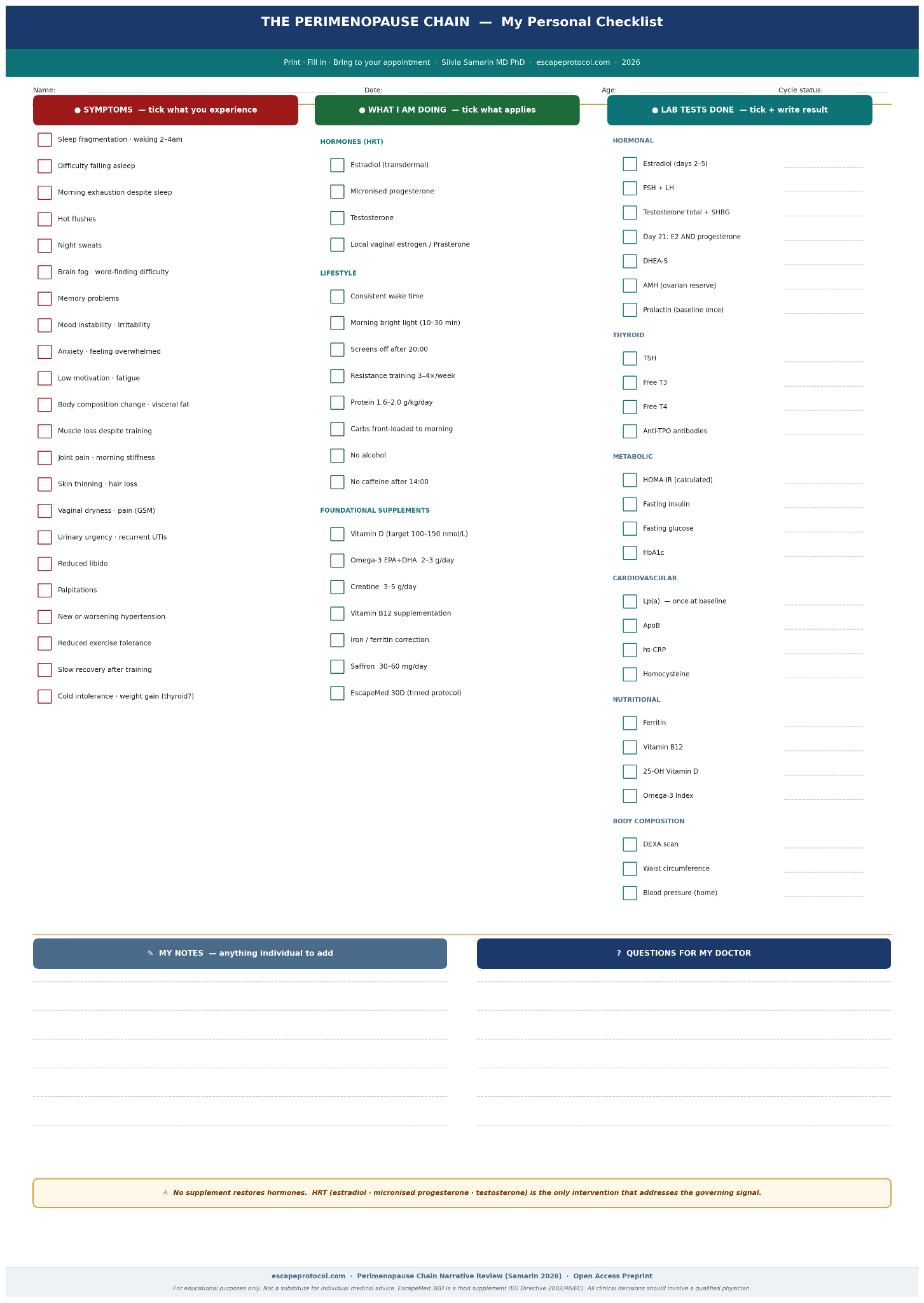
This section is written directly for the perimenopausal woman. It translates the clinical framework of this article into practical actions and the specific questions to ask at any clinical appointment.
| What you feel | What is happening biologically | What to do / what to ask for | Questions to ask your doctor |
|---|---|---|---|
| Sleep fragmentation, waking 2–4am | Neurosteroid withdrawal — progesterone decline (Link 2) | Micronised progesterone (HRT). Super Sleep protocol. Consistent wake time. No alcohol. Bedroom 18°C. | Has micronised progesterone been discussed? Is my serum P monitoring being misinterpreted? |
| Hot flushes, night sweats | Hypothalamic thermoregulation disrupted by estrogen withdrawal (Links 1, 3) | HRT (most effective). Saffron 30–60mg/day (best non-HRT evidence). Alcohol removal. Cooling strategies. | Has HRT been discussed and offered with full safety information? Is the WHI data being misapplied? |
| Body composition change — muscle loss, visceral fat gain | Estrogen and testosterone decline (Links 4, 7) | Resistance training 3–4×/week. Protein 1.6–2.0g/kg/day. Testosterone HRT (primary intervention). Creatine 3–5g/day. DEXA scan. | Has testosterone HRT been discussed? Has a DEXA been done? Is my scale weight being used as a substitute for body composition data? |
| Brain fog, memory difficulty | Sleep disruption + estrogen-dependent neurotransmitter decline (Links 1, 2, 8) | HRT (estradiol + micronised progesterone). Sleep restoration. Omega-3 2–3g/day. Vitamin B12 >300 pmol/L. | Has my sleep quality been assessed? Has B12 been checked against an optimal range (>300, not just >150)? |
| Anxiety, mood instability | Neurosteroid withdrawal — allopregnanolone decline (Links 3, 8) | Micronised progesterone (NOT synthetic progestogen). Estradiol. HPA assessment. Ashwagandha (supportive). | Has my progesterone status been assessed before antidepressants? Is micronised progesterone being used — not a synthetic progestogen? |
| Joint pain, skin changes, hair loss | Estrogen-dependent collagen decline (Link 6) | Estradiol HRT. Collagen cofactor support (timed 08:30–11:00). Protein adequacy. Resistance training. | Has my ferritin been checked? Low ferritin causes hair loss indistinguishable from hormonal hair loss. |
| Vaginal dryness, pain, urinary urgency (GSM) | Local estrogen withdrawal — progressive (Link 6) | Local vaginal estrogen or prasterone (Intrarosa). These are distinct from systemic HRT. Safe in most women. | Has local vaginal estrogen been offered? This is separate from systemic HRT and has a different safety profile. |
| Fatigue despite adequate sleep | Suboptimal ferritin / vitamin D / thyroid — the normal-but-not-optimal gap | Check ferritin (target >50 µg/L), vitamin D (target 100–150 nmol/L), TSH (target 1.0–2.5 mIU/L). | Are my labs being compared to optimal perimenopausal targets — not just standard reference ranges? |
| Still feeling unwell on HRT | Pre-existing circadian disruption. Suboptimal labs. Chain links not yet addressed. | Active circadian rehabilitation (wake time, morning light, meal timing). Recheck ferritin, vitamin D, TSH, HOMA-IR. DEXA if not done. | Has my circadian foundation been assessed? Are my monitoring labs optimal — not just normal? |
Dr. Silvia Samarin, MD, PhD is the founder of Escape Protocol Research and the formulator of EscapeMed 30D. This narrative review includes sections describing EscapeMed 30D as a chronobiological supplementation layer within the M6 intervention framework. All EscapeMed 30D claims are theoretical — based on ingredient-level physiology and mechanism, not controlled clinical trials in perimenopausal populations. EscapeMed 30D is a food supplement (EU Directive 2002/46/EC) and cannot claim to treat, prevent, or cure any condition. All clinical decisions regarding HRT, laboratory testing, and medical intervention should be made with a qualified physician.
Samarin S. (2026). The Perimenopause Chain: A Biological Framework for Understanding and Optimising the Hormonal Transition. Escape Protocol Research. Preprint. Open access. escapeprotocol.com/perimenopause-chain.html
- Bannai M, Kawai N. (2012). Glycine improves the quality of sleep. Journal of Pharmacological Sciences, 118(2), 145–148.
- Barbagallo M, et al. (2001). Role of magnesium in insulin action, diabetes and cardio-metabolic syndrome X. Molecular Aspects of Medicine, 22(1–3), 49–69.
- Brinton RD. (2009). Estrogen-induced plasticity from cells to circuits. Trends in Pharmacological Sciences, 30(4), 212–222.
- Brzezinski A, et al. (2005). Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Medicine Reviews, 9(1), 41–50.
- Canonico M, et al. (2010). Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism. Arteriosclerosis, Thrombosis, and Vascular Biology, 30(2), 340–345.
- Chlebowski RT, et al. (2003). Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the WHI randomised trial. JAMA, 289(24), 3243–3253.
- Colditz GA, et al. (2012). Cumulative risk of breast cancer to age 70 years according to risk factor status. British Journal of Cancer, 106(4), 819–824.
- Davis SR, et al. (2019). Global consensus position statement on testosterone therapy for women. Journal of Clinical Endocrinology & Metabolism, 104(10), 4660–4666.
- Dou X, et al. (2017). Short-term rapamycin treatment increases ovarian lifespan in young and middle-aged female mice. Aging Cell, 16(4), 825–836.
- El Khoudary SR, et al. (2020). Menopause transition and cardiovascular disease risk. Circulation, 142(25), e506–e532.
- Fournier A, et al. (2008). Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Research and Treatment, 107(1).
- Jia F, et al. (2008). Taurine is a potent activator of extrasynaptic GABA-A receptors in the thalamus. Journal of Neuroscience, 28(1), 106–115.
- Nordestgaard BG, et al. (2010). Lipoprotein(a) as a cardiovascular risk factor. European Heart Journal, 31(23), 2844–2853.
- Roenneberg T, et al. (2012). Social jetlag and obesity. Current Biology, 22(10), 939–943.
- Samarin S. (2026). The EscapeMed 30D System: Signal Logic, Dose Rationale, and Pilot Evidence. Escape Protocol Research. Preprint.
- Takahashi JS. (2017). Transcriptional architecture of the mammalian circadian clock. Nature Reviews Genetics, 18, 164–179.
- Thornton MJ. (2013). Estrogens and aging skin. Dermato-Endocrinology, 5(2), 264–270.
- Villaseca P. (2012). Non-estrogen conventional and phytochemical treatments for vasomotor symptoms. Climacteric, 15(2), 115–137.
- Zhang R, et al. (2024). Sleep and biological aging. eLife, 13, e88031.
- Zhao J, et al. (2021). Efficacy of saffron supplementation in menopausal women: a systematic review. Phytomedicine, 90, 153631.