Every morning, millions of people wake up, glance at a wrist or finger device, and read a number that tells them how recovered they are. That number — heart rate variability — has become one of the most talked-about metrics in performance optimisation. The premise is simple: higher is better. Stress reduces it. Sleep and recovery increase it. Train smarter, sleep deeper, manage your cortisol, and you will drive it up.
Except that for a meaningful fraction of the population, this is not fully true. Their HRV is low not because something is wrong, not because they are doing something suboptimal, but because their biology — their autonomic wiring, their cardiac genomics — is calibrated differently. This is the story of constitutional low HRV.
What Is Heart Rate Variability
Heart rate variability is not a measure of how fast your heart beats. It is a measure of how irregularly it beats — specifically, how much the time between consecutive heartbeats varies from one beat to the next.
The sinus node: your heart's pacemaker
Deep in the right atrium of the heart sits a small cluster of specialised cells called the sinus node — the sinoatrial node. This structure is the heart's intrinsic pacemaker. Left entirely to itself, in a completely isolated heart with no external input, the sinus node would fire at a steady rate of roughly 60–100 beats per minute. Every beat would arrive exactly on schedule. Beat-to-beat variation would be minimal.
But the heart is not isolated. It is continuously being modulated by the autonomic nervous system — the part of the nervous system that operates largely outside conscious control, governing everything from digestion to pupil diameter to cardiac output. Through two opposing branches, the autonomic nervous system reaches the sinus node at every moment and either accelerates or decelerates it.
Two branches, one organ
The sympathetic nervous system is the accelerator. It releases noradrenaline onto the sinus node, increasing heart rate and reducing the gap between beats. This is the system activated during stress, exercise, and any state that requires increased output. Sympathetic dominance produces a faster, more regular heartbeat — and paradoxically, less variability between beats.
The parasympathetic nervous system — delivered to the heart primarily through the vagus nerve — is the brake. It releases acetylcholine onto the sinus node, slowing the heart rate. Under parasympathetic dominance, the heart slows and becomes more irregular, responding dynamically to each breath, each shift in blood pressure, each cognitive state.
HRV is therefore a proxy for autonomic balance, and particularly for vagal tone. A person with high HRV has a heart that is highly responsive to parasympathetic input. A person with low HRV has a heart that is less responsive to this modulation, tending toward a steadier, less flexible rhythm.
HRV is measured in milliseconds — the variation in the interval between consecutive R-wave peaks on the ECG (R-R intervals). The most widely used metric in wearable devices is RMSSD: the root mean square of successive differences between adjacent R-R intervals. RMSSD reflects short-term parasympathetic activity and is the number your WHOOP and Oura Ring report each morning.
What HRV measures in clinical practice
In clinical cardiology, HRV has been studied since the 1980s, when it was first established as a predictor of post-infarction mortality — a window into the health and adaptability of the autonomic nervous system itself. In the broader literature, low HRV has been associated with increased cardiovascular morbidity and mortality in at-risk populations, higher psychological stress load, impaired physical recovery, metabolic dysfunction, inflammatory states, and ageing. High HRV is associated with cardiovascular resilience, good recovery capacity, emotional regulation, and physiological adaptability.
When HRV Does Not Apply: The Arrhythmia Exception
Heart rate variability is only meaningful in normal sinus rhythm. In the presence of common cardiac arrhythmias — including atrial fibrillation and frequent ectopic beats — HRV values from consumer wearables become unreliable or actively misleading. This is a fundamental limitation that is almost never communicated to users.
This point requires emphasis, because tens of millions of people worldwide carry cardiac arrhythmias and many use HRV-based recovery tools without any awareness of this limitation.
Atrial fibrillation
In atrial fibrillation (AF) — the most common sustained cardiac arrhythmia, affecting an estimated 33–43 million people globally — the sinus node no longer controls heart rhythm. Instead, chaotic electrical activity in the atria produces an irregularly irregular ventricular response. The R-R intervals are highly variable, but this variability has nothing to do with autonomic modulation. It is intrinsic electrical chaos.
A person in AF will typically register very high HRV on a consumer device — not because they are well-recovered, but because the algorithm is interpreting atrial electrical disorder as parasympathetic richness. The number is artifactually inflated and completely uninterpretable from an autonomic standpoint.
Frequent ectopic beats
Premature atrial contractions (PACs) and premature ventricular contractions (PVCs) introduce anomalous short R-R intervals followed by compensatory pauses. Even a small proportion of ectopic beats within a measurement window can substantially distort RMSSD calculations. Consumer devices vary widely in their ability to detect and exclude ectopic beats from HRV analysis.
The clinical implication: if you have known AF, frequent ectopics, or any other rhythm disorder, your HRV numbers from a wrist or finger device should be interpreted with extreme caution, and ideally in consultation with a cardiologist. The metric was designed for, and is validated in, normal sinus rhythm. This is also the reason that artefact removal is a necessary step in any serious analysis of long-term wearable HRV data — as demonstrated in the case below.
How Common Is Low HRV — and Where Does Constitutional Low HRV Fit
The optimisation industry implicitly assumes that everyone begins at the same starting point and that HRV responds to the same inputs in the same way. This model is partially correct, but it ignores a fundamental reality: HRV is a highly heritable, highly individual trait with a wide normal distribution, and a substantial proportion of the population sits chronically at the lower end regardless of behavioural optimisation.
| Parameter | Finding |
|---|---|
| Heritability of resting RMSSD | 30–50% (twin study estimates) — at minimum one-third of your baseline HRV is determined by your genome |
| Constitutional low HRV prevalence | Approximately 20–25% of adults consistently in the lowest HRV quartile regardless of training status or lifestyle optimisation |
| Age-related decline | Approximately 1 ms per year of RMSSD from age 30 onward; population mean for women aged 54 is approximately 25–38 ms |
| Sex effect | Females have modestly higher HRV before menopause; this advantage is reduced or reversed after menopause, likely due to loss of oestrogen's cardioprotective effects on vagal tone |
| Genetic architecture | GWAS analyses (UK Biobank, n > 23,000; van den Berg et al., 2020, Nature Genetics) have identified dozens of loci associated with resting HRV |
Population distribution of HRV. Data from published literature including van den Berg et al. (2020) GWAS and Task Force of the European Society of Cardiology (1996) standards.
People with constitutional low HRV often work harder on optimisation protocols precisely because they feel something is wrong. They sleep more, meditate more, reduce training load, add recovery tools — and their HRV remains low. The feedback loop creates anxiety, which further activates the sympathetic nervous system, which further suppresses HRV. This is not a failure of the person. It is a failure of the framework to account for biological individuality.
What drives constitutional low HRV
Reduced vagal tone
Some individuals have intrinsically lower parasympathetic drive to the sinus node, possibly related to differences in vagal nucleus activity or cardiac innervation density.
Altered beta-adrenergic receptor sensitivity
Variants in genes encoding adrenergic receptors (such as ADRB2) affect how the sinus node responds to sympathetic input, influencing the sympathovagal balance at rest.
Differences in GPCR regulation kinetics
G-protein coupled receptor kinases (GRKs) regulate how quickly cardiac adrenergic receptors are desensitised after activation. Variants in GRK5 — the only cardiac GRK with clinically characterised genetic polymorphisms — alter the gain and timing of adrenergic signal termination.
Perimenopause and ageing
Both ageing and hormonal transition reduce vagal tone and increase sympathetic baseline, lowering HRV in ways that no protocol fully reverses.
The Case: 834 Nights, Two Devices, One Question
Subject: Female, 54 years, MD PhD, cardiologist. Morning chronotype. Perimenopausal. Active lifestyle, no cardiac disease, no diagnosed arrhythmia. Whole-genome sequencing April 2024 (Dante Labs, Kit ID GFX0455821).
Devices: WHOOP 4.0 (wrist, 5-minute sleep window RMSSD) + Oura Ring Gen 3 (finger, nightly RMSSD), worn simultaneously since December 2023.
Clinical question: Is chronically low HRV — documented across 834 clean nights on two independent devices — explained by lifestyle, fitness level, age, and perimenopause alone, or does it represent a constitutional genomic phenotype?
Artifact removal and data quality
Six nights were excluded from analysis due to anomalously high HRV readings (range 54–88 ms) combined with very low recovery scores (6–12%). This specific combination — high measured variability, poor recovery — is the characteristic signature of R-R interval contamination by ectopic beats or brief arrhythmic episodes, which inflate RMSSD calculation without reflecting true autonomic richness. All six were isolated nights with no preceding or following elevation, consistent with measurement artefact rather than genuine autonomic change. After exclusion, the clean dataset comprises 834 nights.
What the data shows
| Metric | Value | Context |
|---|---|---|
| Mean RMSSD (WHOOP) | 19.8 ms | Population mean for women 54yo: ~30 ms |
| Median RMSSD | 19.0 ms | Below 10th population percentile for age |
| SD | 4.3 ms | Narrow range — low variability around a low mean |
| True range (clean) | 9–41 ms | Maximum ever recorded: 41 ms |
| Nights below 20 ms | 54% (447/834) | Majority of nights below the lower constitutional threshold |
| Nights above 30 ms | 3% (24/834) | Rarely reaches population median |
| Nights above 38 ms | 1% (8/834) | Almost never reaches population mean |
| Oura Ring mean RMSSD | 16.3 ms | Independent device confirmation, lower due to whole-night averaging |
| Both devices <30 ms | 92% of matched nights | Dual-device concordance on constitutional low HRV |
834 clean nights of dual-device RMSSD data. 6 artifact nights excluded (anomalously high HRV + very low recovery = ectopic beat signature).
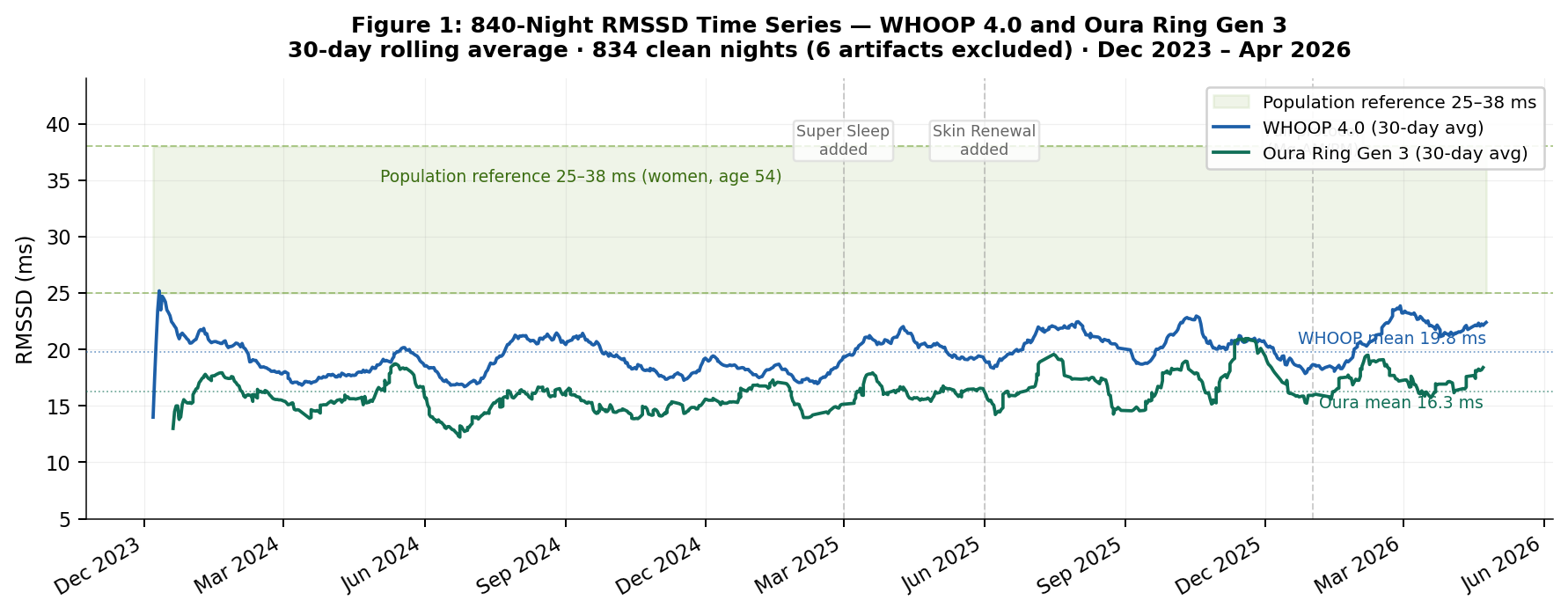
Figure 1. 840-Night RMSSD Time Series — WHOOP 4.0 and Oura Ring Gen 3. 30-day rolling average · 834 clean nights (6 artifacts excluded) · December 2023 – April 2026. Population reference band (25–38 ms, women age 54) shaded. Both devices remain consistently below the reference range across the full observation period regardless of phase, season, or supplement changes. WHOOP mean 19.8 ms · Oura mean 16.3 ms.
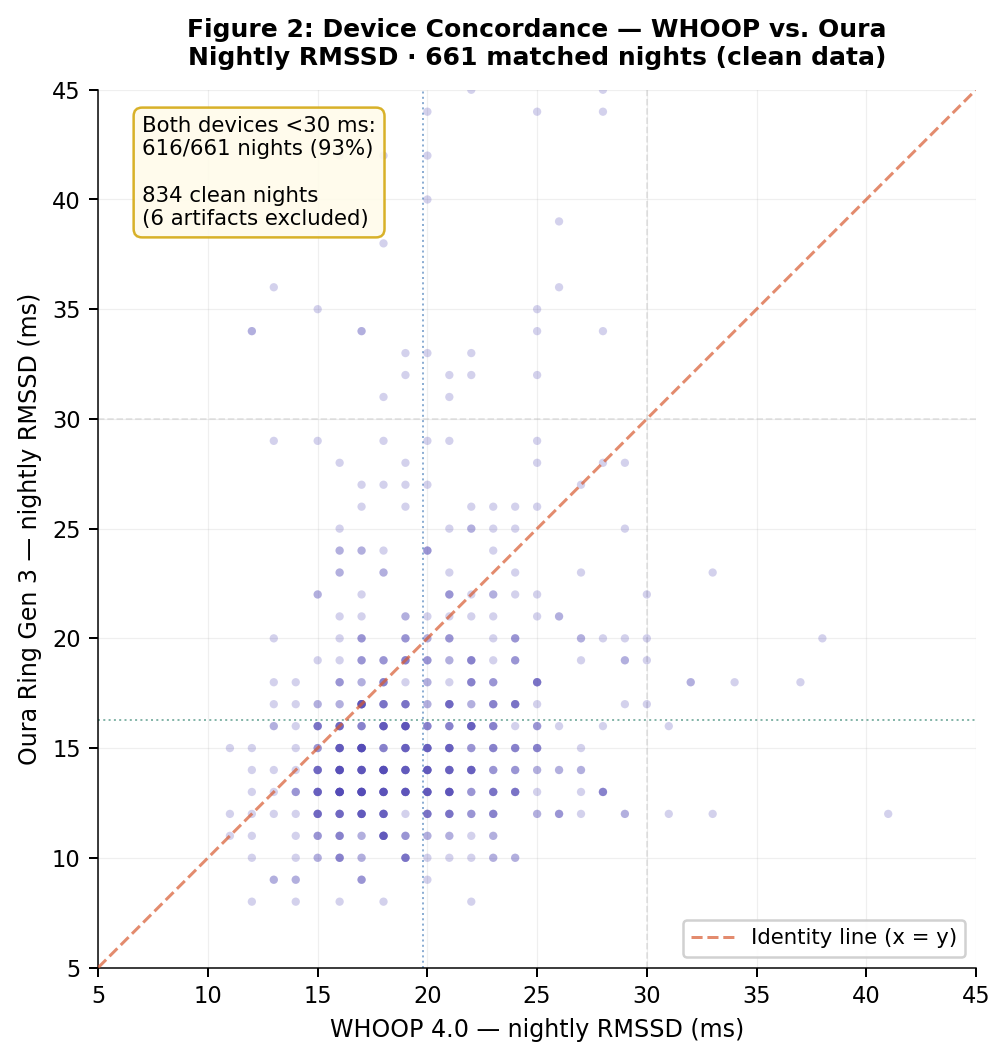
Figure 2. Device Concordance — WHOOP vs. Oura Ring · 661 matched clean nights. Both devices measure independently using different sensor wavelengths and anatomical placements. The low direct correlation (r = 0.12) reflects different measurement protocols (5-minute deep sleep window vs. whole-night average), not disagreement: both independently confirm low HRV across the full range. 616 of 661 matched nights (93%): both devices below 30 ms simultaneously.
HRV and recovery: within-person correlation
After artifact removal, the Pearson correlation between nightly RMSSD and recovery score is r = 0.683 — a strong positive association across 834 nights. This is substantially higher than the raw pre-cleaning correlation of r = 0.34, which was distorted by the six artifact nights. The tertile analysis illustrates the practical implication:
| HRV Tertile (WHOOP) | Mean Recovery Score | Interpretation |
|---|---|---|
| Low: ≤18 ms (bottom third) | 47.5% | Below recommended training threshold |
| Mid: 18–21 ms (middle third) | 66.6% | Moderate recovery, trainable range |
| High: >21 ms (top third) | 79.1% | Good recovery — still below population average |
Within-person HRV tertile vs. recovery score (834 clean nights). Even within a constitutionally low range, the relative variation carries strong predictive signal.
Even within a constitutionally low HRV range, the within-person variation carries strong predictive signal for recovery. The practical implication: for this individual, HRV is more useful as a relative indicator (deviation from personal baseline) than as an absolute number compared against population norms.
Supplement phase analysis
The 840-night observation period encompasses four distinct supplement protocol phases, allowing an exploratory assessment of whether structured supplementation was associated with any change in HRV metrics. This is an N=1 observational analysis — no causal inference is possible.
| Phase | Period | N nights | Mean HRV | Nights <20 ms | Mean recovery |
|---|---|---|---|---|---|
| 1 — No EscapeMed 50+ individual supplements | Dec 2023–Feb 2025 | 445 | 18.9 ms | 62% | 62.1% |
| 2 — + Super Sleep | Mar–May 2025 | 85 | 20.1 ms | 51% | 61.4% |
| 3 — + Skin Renewal | Jun–Dec 2025 | 201 | 20.5 ms | 48% | 62.0% |
| 4 — Full protocol + Magnesium AM/PM | Jan–Apr 2026 | 103 | 21.8 ms | 30% | 65.1% |
Four supplement phases. Directional trend present but ceiling unchanged. Constitutional setpoint not reversed.
A directional trend is present: mean HRV increased incrementally across phases, and the proportion of nights below 20 ms fell from 62% to 30% between Phase 1 and Phase 4. This is consistent with the sleep architecture findings reported in the companion case report. However, the ceiling did not change — the maximum recorded HRV remained below 41 ms throughout all phases. Constitutional low HRV was not reversed. What changed was the distribution: fewer very low nights, higher mean, better recovery correlation in the final phase. The most parsimonious interpretation is that structured supplementation improved the signal quality — reducing the frequency of lowest-tier nights — without altering the genomically-anchored setpoint.
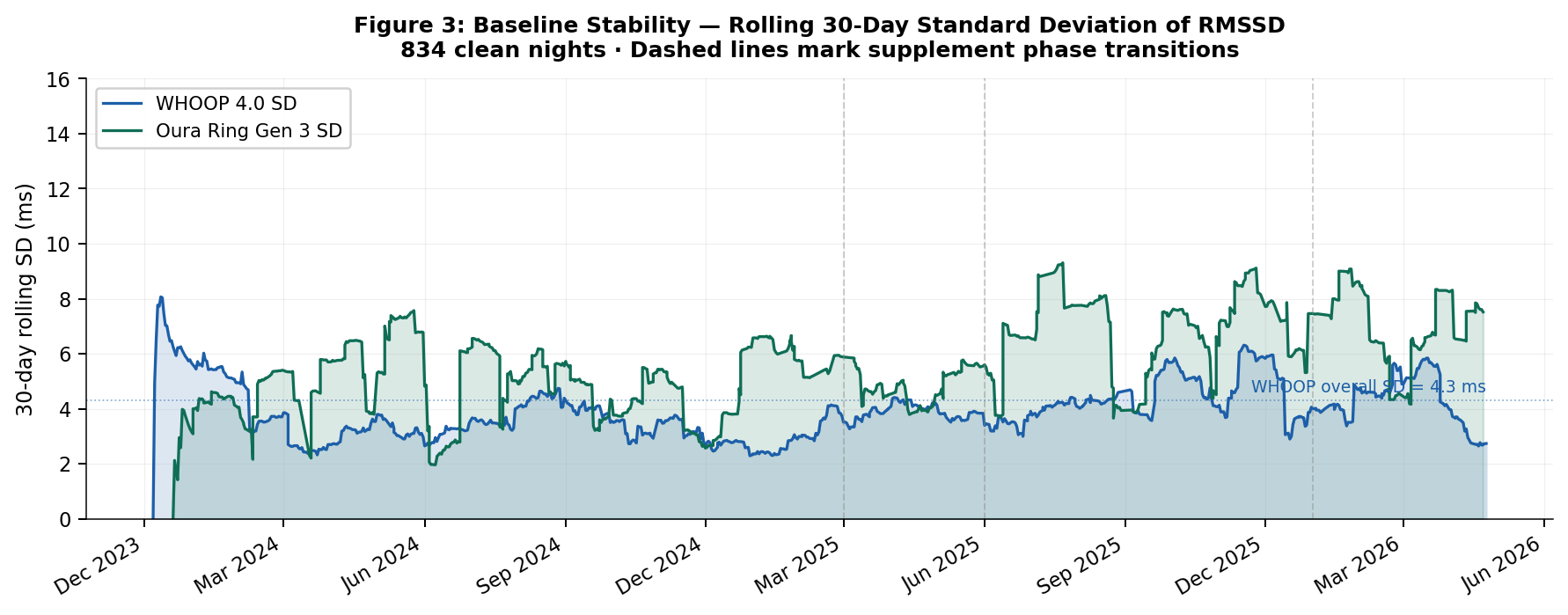
Figure 3. Personal Baseline Stability — Rolling 30-Day Standard Deviation of RMSSD · 834 clean nights. Dashed lines mark supplement phase transitions. The rolling SD remains consistently narrow across all phases, seasons, and supplement changes — demonstrating stability of the constitutional setpoint independent of behavioural variation. WHOOP overall SD = 4.3 ms.
The Genomic Context
Whole-genome sequencing identified two variants with direct functional relevance to HRV phenotype, and confirmed structural integrity of the major cardiac ion channels:
Altered GPCR desensitisation kinetics. GRK5 is the only cardiac GRK with clinically characterised genetic variation. Affects speed and gain of β-adrenergic receptor downregulation after sympathetic activation. Influences cardiac performance modulation; altered adrenergic receptor cycling dynamics affect sinus node responsiveness.
Arg16Gly substitution in β2-adrenergic receptor. Arg16 carriers show altered agonist-promoted downregulation. Published literature documents lower sympathetic HRV indices in Arg16 carriers vs. Gly16 homozygotes. Directly affects sympathovagal balance through altered β2-receptor signalling; documented HRV effect in multiple human studies.
Pacemaker current (If), slow delayed rectifier (IKs), and cardiac sodium channel structurally normal. Major structural ion channel architecture intact — low HRV is not explained by ion channel pathology.
The combination of a homozygous GRK5 variant and a heterozygous ADRB2 Arg16Gly variant provides a plausible genomic architecture for chronically reduced HRV. Neither variant is pathological. Neither produces disease. Both modulate the gain and dynamics of the autonomic signalling system in ways that, in aggregate, shift the HRV setpoint downward.
Chronically low HRV in this case is not a signal of cardiovascular disease, autonomic failure, or inadequate recovery practice. It is a constitutional phenotype — a genomically-anchored biological setpoint. The appropriate response is not to escalate optimisation protocols, but to recalibrate the interpretation framework: what matters is not the absolute number relative to population norms, but the directional signal relative to the individual's own stable baseline.
What This Means If You Are Reading Your Own Number
Consumer HRV tracking has genuine value. It captures real biological signal. The problem is not the measurement — it is the narrative that has been built around it. The five questions below are the ones most commonly asked by people who have been tracking their HRV for months and cannot make the number do what the optimisation industry promised it would do.
The key marker is time and stability. A low HRV that persists across at least six months — across different sleep conditions, stress loads, training cycles, and seasons — without recovering toward population norms is a constitutional signal. One bad week is not a diagnosis. A brief dip after illness, overtraining, or alcohol is expected and reversible. But if your rolling 30-day average has been in the same narrow range for 400, 600, 800 nights regardless of what you optimise, you are most likely looking at your baseline, not a temporary deficit.
The dual-device test adds confidence: if two independently measuring devices (wrist and finger, using different algorithms) both consistently record low values, device artefact is ruled out. The finding is real.
This is the question people are most afraid to ask, and the answer requires a careful distinction that the popular literature almost never makes. The mortality association with low HRV comes from studies of post-infarction patients and individuals with established cardiovascular disease. In these populations, very low HRV is a marker of impaired cardiac autonomic recovery after damage — and it does predict worse outcomes. This finding does not automatically transfer to otherwise healthy individuals with a stable constitutional baseline and no cardiac disease.
In healthy people, chronically low HRV without cardiac disease, without autonomic dysfunction, and without new decline is not associated with shortened lifespan in the published evidence. A cardiologist looking at a 54-year-old with normal cardiac anatomy, no arrhythmia, no structural disease, and a stable RMSSD of 20 ms does not see a cardiovascular risk signal. She sees a constitutional variant.
What does carry risk is new, declining, symptomatic low HRV — particularly if accompanied by palpitations, syncope, breathlessness, or known cardiac disease. Stable and longstanding is a different biological category entirely.
The honest answer, not the optimisation industry answer:
- Aerobic fitness sustained over months has real evidence for modestly raising resting HRV — through autonomic remodelling, not acute effect
- Sleep consistency (same bedtime, protecting deep sleep) reduces the frequency of lowest-tier nights without necessarily raising the mean
- Breathing practices (slow diaphragmatic breathing, box breathing) produce temporary acute increases in HRV that do not persist as resting baseline change
- Supplementation addressing magnesium deficiency, autonomic nervous system support, and sleep architecture may improve the distribution of HRV nights — fewer very low readings — as observed in this case
- Alcohol reliably suppresses HRV the following night — removing it produces the most consistent single behavioural improvement
What does not reliably raise constitutional low HRV: meditation alone, one good night of sleep, generic stress management without addressing the underlying autonomic setpoint, or any intervention over days to weeks in someone with a genomically-anchored baseline.
Not everyone with constitutional low HRV will find a clear explanation in whole-genome sequencing. Identified variants explain part of the variance, not all of it. Constitutional low HRV can exist without an identifiable genomic cause for several reasons:
- Reduced cardiac innervation density may be a developmental characteristic not captured by current variant catalogues
- Altered vagal nucleus activity in the brainstem may reflect subtle neuroanatomical variation not yet genotyped at population scale
- The perimenopausal autonomic shift accounts for a real and documented HRV decline that may be the primary driver in some individuals
- Population-normal variation at the lower end of a wide distribution is sufficient — not everyone at the 10th percentile has a pathological explanation for being there
The absence of an identified variant does not mean the finding is not constitutional. It means the mechanism is not yet characterised at the genetic level. The clinical interpretation remains the same: stable, longstanding, asymptomatic low HRV in a person without cardiac disease is not a pathological finding.
Low HRV is worth formal evaluation when:
- It is new and declining — not a stable longstanding pattern but a recent change from a previously normal range
- It is accompanied by symptoms: palpitations, unexplained fatigue, exercise intolerance, presyncope, or syncope
- It occurs in the context of known cardiac disease, diabetes, or other conditions with documented autonomic complications
- The wearable repeatedly flags possible arrhythmia detection alongside the low HRV readings
- It is accompanied by very low resting HRV on a formal 24-hour Holter monitor, not just a consumer wearable
Stable constitutional low HRV in an asymptomatic person with normal cardiac history, stable readings across years, and no arrhythmia signals does not require investigation. It requires informed interpretation.
The Practical Conclusion
If your HRV is low, has always been low, does not change substantially with optimisation, and you have no cardiac symptoms — the most useful reframe is this: your number is not broken. Your device is measuring your biology accurately. What needs to change is not your HRV, but your interpretation framework. Track deviation from your personal baseline. Pay attention to the floor rising, not just the ceiling. And if you have access to whole-genome sequencing, the autonomic signalling genes are worth examining — they may show you exactly why your system is calibrated the way it is.
The 840-night data in this case shows exactly this: structured supplementation moved the floor upward and reduced the proportion of lowest-tier nights from 62% to 30%, while the ceiling remained below 41 ms throughout. The setpoint did not shift. The signal quality improved. Both findings matter — and understanding which one is achievable is the difference between a useful framework and an endless cycle of futile optimisation.
The author is founder of EscapeMed d.o.o. and the Escape Protocol Research platform. This article describes an N=1 observational case and should not be interpreted as clinical advice. Genomic variants cited are from whole-genome sequencing (Dante Labs, April 2024, Kit ID GFX0455821) and are referenced in the context of published scientific literature. WHOOP 4.0 and Oura Ring Gen 3 are commercial devices; the author has no financial relationship with either company. All EscapeMed supplement products are food supplements under EU Regulation 1924/2006; claims have not been evaluated by EFSA for disease treatment or prevention.
Samarin, S. (2026). Chronically Low HRV: Constitutional Phenotype or Correctable Problem? Genomics, Autonomic Architecture, and 840 Nights of Dual-Device Evidence. Escape Protocol Research. Preprint. escapeprotocol.com/low-hrv.html
- van den Berg M.E. et al. (2020). Genome-wide association study of heart rate variability. Nature Genetics. UK Biobank, n > 23,000.
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (1996). Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation, 93(5), 1043–1065.
- Thayer J.F. & Lane R.D. (2007). The role of vagal function in the risk for cardiovascular disease and mortality. Biological Psychology, 74(2), 224–242.
- La Rovere M.T. et al. (1998). Baroreflex sensitivity and heart rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI study. Lancet, 351(9101), 478–484.
- Leosco D. et al. GRK5 and cardiac function — multiple publications on GRK5 cardiac role and genetic variation.
- Drysdale C.M. et al. ADRB2 Arg16Gly functional consequences — published literature on beta-2 adrenergic receptor polymorphism and sympathovagal balance.
- Sammain S. (2026). Better Deep Sleep Under More Stress: Behind the Paradox. N=1 Case Report. Escape Protocol Research. Preprint. escapeprotocol.com/better-deep-sleep.html